

Baricitinib restrains the immune dysregulation in patients with severe COVID-19
- PMID: 32809969
- PMCID: PMC8016181
- DOI: 10.1172/JCI141772
Baricitinib restrains the immune dysregulation in patients with severe COVID-19
Abstract
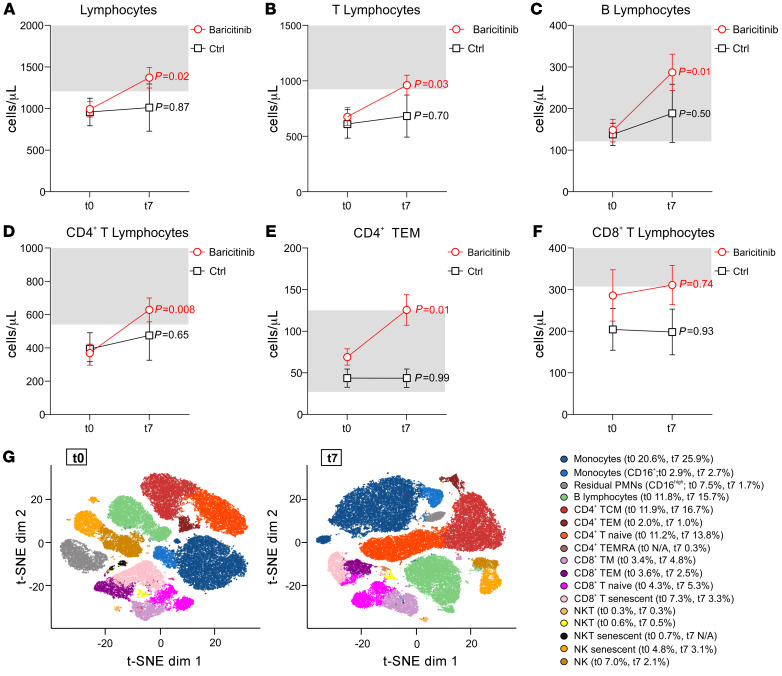
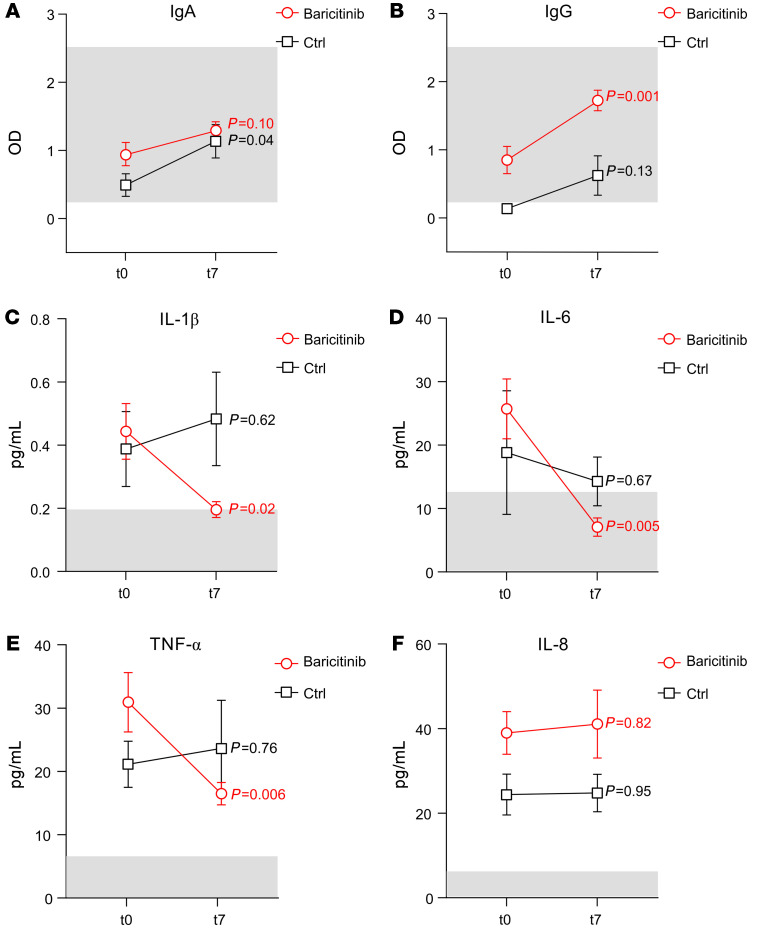
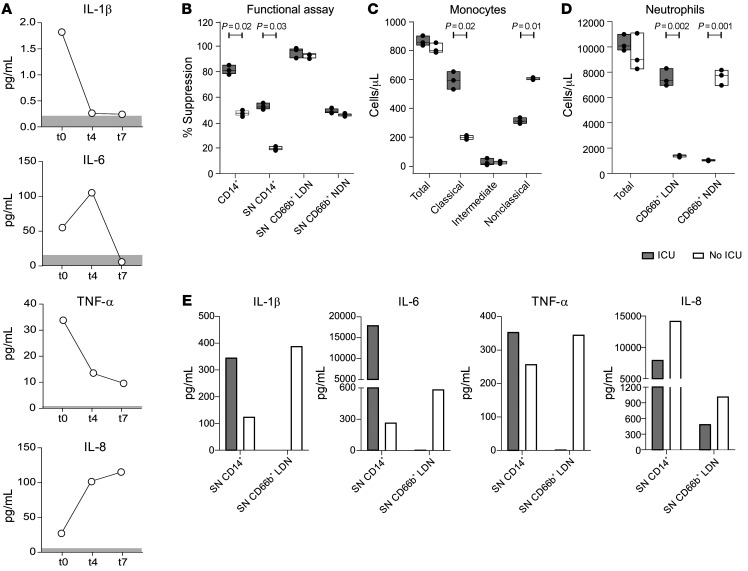
BACKGROUNDPatients with coronavirus disease 2019 (COVID-19) develop pneumonia generally associated with lymphopenia and a severe inflammatory response due to uncontrolled cytokine release. These mediators are transcriptionally regulated by the JAK/STAT signaling pathways, which can be disabled by small molecules.METHODSWe treated a group of patients (n = 20) with baricitinib according to an off-label use of the drug. The study was designed as an observational, longitudinal trial and approved by the local ethics committee. The patients were treated with 4 mg baricitinib twice daily for 2 days, followed by 4 mg per day for the remaining 7 days. Changes in the immune phenotype and expression of phosphorylated STAT3 (p-STAT3) in blood cells were evaluated and correlated with serum-derived cytokine levels and antibodies against severe acute respiratory syndrome-coronavirus 2 (anti-SARS-CoV-2). In a single treated patient, we also evaluated the alteration of myeloid cell functional activity.RESULTSWe provide evidence that patients treated with baricitinib had a marked reduction in serum levels of IL-6, IL-1β, and TNF-α, a rapid recovery of circulating T and B cell frequencies, and increased antibody production against the SARS-CoV-2 spike protein, all of which were clinically associated with a reduction in the need for oxygen therapy and a progressive increase in the P/F (PaO2, oxygen partial pressure/FiO2, fraction of inspired oxygen) ratio.CONCLUSIONThese data suggest that baricitinib prevented the progression to a severe, extreme form of the viral disease by modulating the patients' immune landscape and that these changes were associated with a safer, more favorable clinical outcome for patients with COVID-19 pneumonia.TRIAL REGISTRATIONClinicalTrials.gov NCT04438629.FUNDINGThis work was supported by the Fondazione Cariverona (ENACT Project) and the Fondazione TIM.
Keywords: COVID-19; Immunology; Innate immunity.
Conflict of interest statement
Figures
Comment in
-
Caring for patients in a new pandemic: the necessity and challenges of observational research.J Clin Invest. 2020 Dec 1;130(12):6225-6227. doi: 10.1172/JCI143292. J Clin Invest. 2020. PMID: 32902413 Free PMC article.
References
-
- World Health Organization. Coronavirus disease (COVID-19) outbreak. https://www.who.int Accessed June 26, 2020.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
