

Systematic review and meta-analysis of the effectiveness of pre-pregnancy care for women with diabetes for improving maternal and perinatal outcomes
- PMID: 32810195
- PMCID: PMC7433888
- DOI: 10.1371/journal.pone.0237571
Systematic review and meta-analysis of the effectiveness of pre-pregnancy care for women with diabetes for improving maternal and perinatal outcomes
Abstract
Background: Pre-gestational diabetes mellitus is associated with increased risk of maternal and perinatal adverse outcomes. This systematic review was conducted to evaluate the effectiveness and safety of pre-conception care (PCC) in improving maternal and perinatal outcomes.
Methods: Databases from MEDLINE, EMBASE, WEB OF SCIENCE, and Cochrane Library were searched, including the CENTRAL register of controlled trials, and CINHAL up until March 2019, without any language restrictions, for any pre-pregnancy care aiming at health promotion, glycemic control, and screening and treatment of diabetes complications in women with type I or type II pre-gestational diabetes. Trials and observational studies were included in the review. Newcastle-Ottawa scale and the Cochrane collaboration methodology for data synthesis and analysis were used, along with the GRADE tool to evaluate the body of evidence.
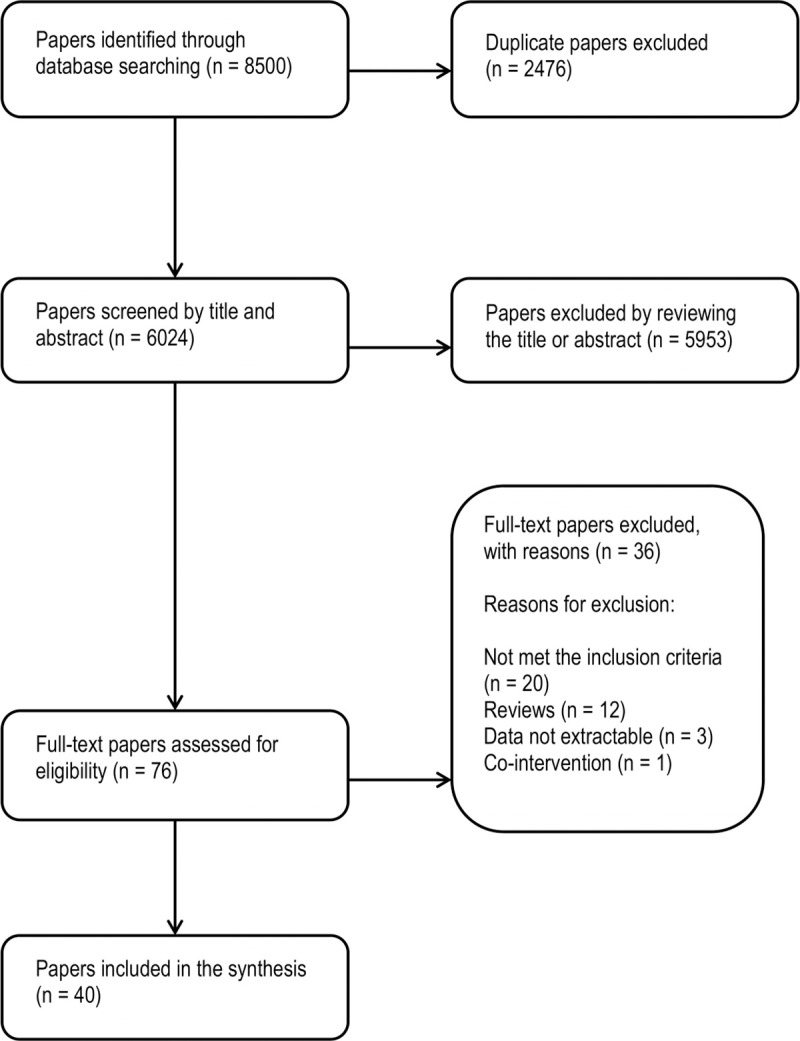
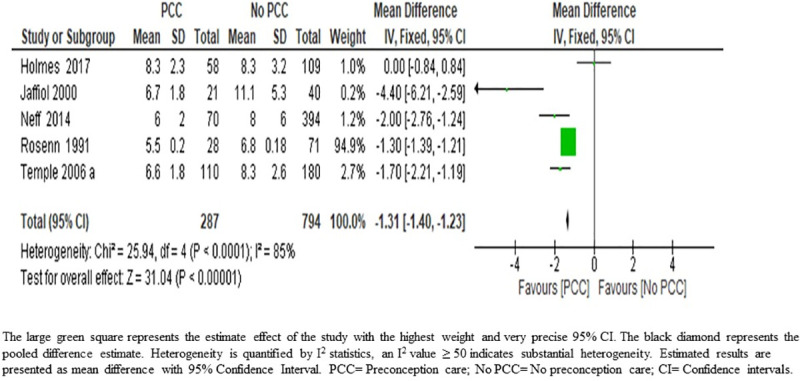
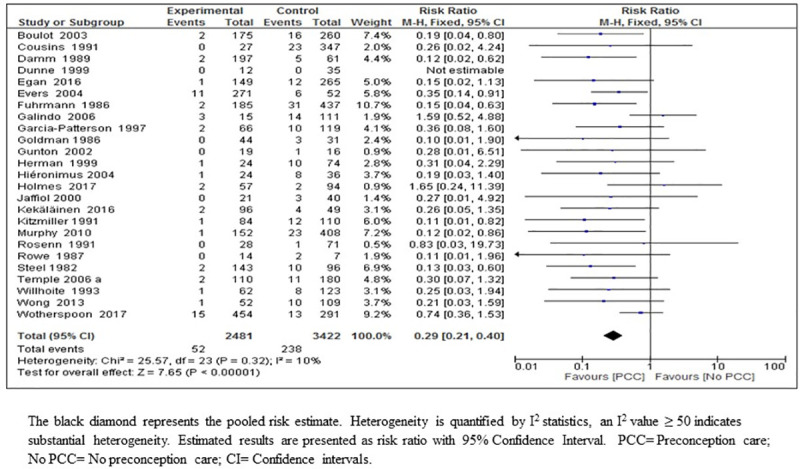
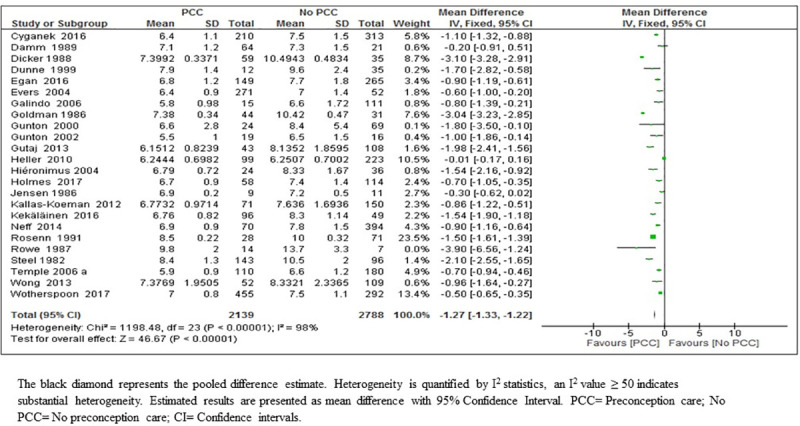
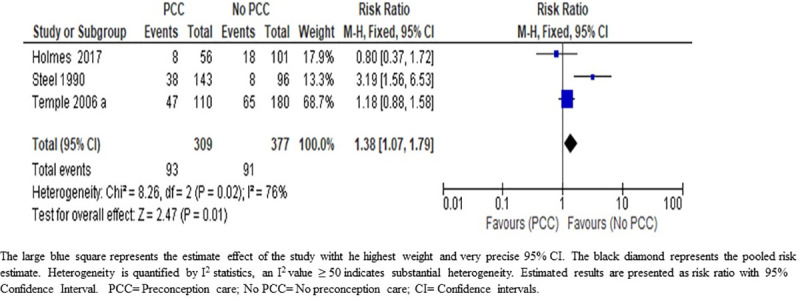
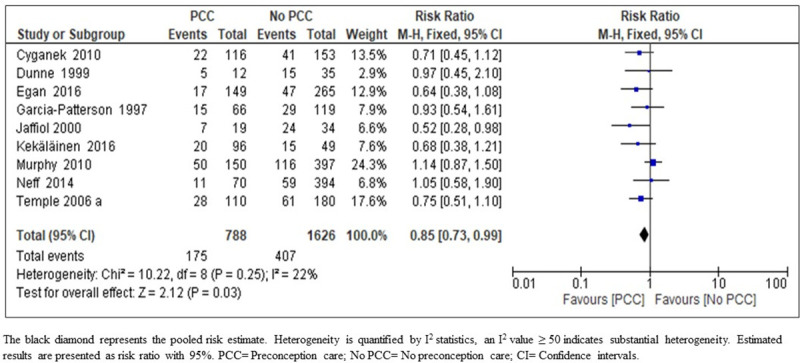
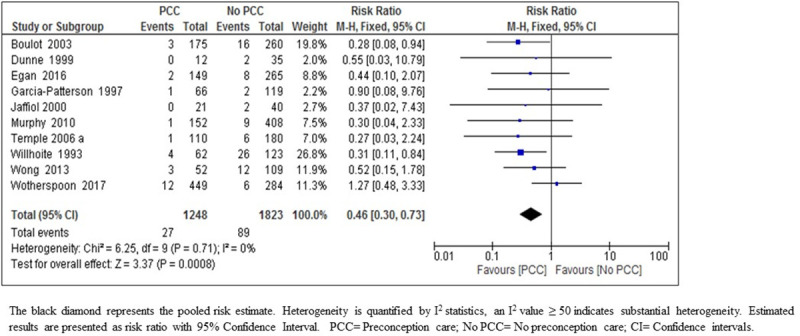
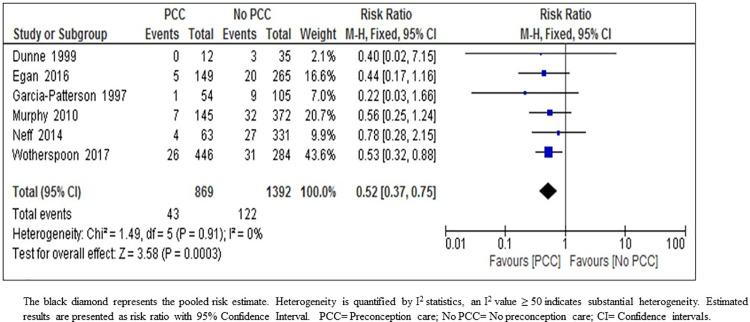
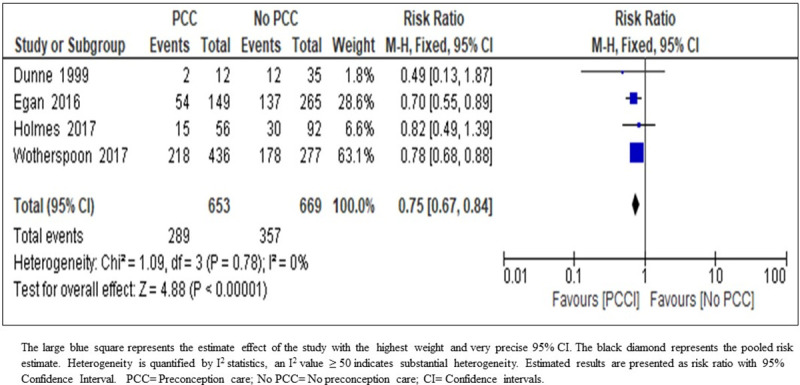
Results: The search identified 8500 potentially relevant citations of which 40 reports of 36 studies were included. The meta-analysis results show that PCC reduced congenital malformations risk by 71%, (Risk ratio (RR) 0.29; 95% CI: 0.21-0.40, 25 studies; 5903 women; high-certainty evidence). The results also show that PCC may lower HbA1c in the first trimester of pregnancy by an average of 1.27% (Mean difference (MD) 1.27; 95% CI: 1.33-1.22; 4927 women; 24 studies, moderate-certainty evidence). Furthermore, the results suggest that PCC may lead to a slight reduction in the risk of preterm delivery of 15%, (RR 0.85; 95% CI: 0.73-0.99; nine studies, 2414 women; moderate-certainty evidence). Moreover, PCC may result in risk reduction of perinatal mortality by 54%, (RR 0.46; 95% CI: 0.30-0.73; ten studies; 3071 women; moderate-certainty evidence). There is uncertainty about the effects of PCC on the early booking for antenatal care (MD 1.31; 95% CI: 1.40-1.23; five studies, 1081 women; very low-certainty evidence) and maternal hypoglycemia in the first trimester, (RR 1.38; 95% CI: 1.07-1.79; three studies; 686 women; very low- certainty evidence). In addition, results of the meta-analysis indicate that PCC may lead to 48% reduction in the risk of small for gestational age (SGA) (RR 0.52; 95% CI: 0.37-0.75; six studies, 2261 women; moderate-certainty evidence). PCC may reduce the risk of neonatal admission to intensive care unit (NICU) by 25% (RR 0.75; 95% CI: 0.67-0.84; four studies; 1322 women; moderate-certainty evidence). However, PCC may have little or no effect in reducing the cesarean section rate (RR 1.02; 95% CI: 0.96-1.07; 14 studies; 3641 women; low-certainty evidence); miscarriage rate (RR 0.86; 95% CI: 0.70-1.06; 11 studies; 2698 women; low-certainty evidence); macrosomia rate (RR 1.06; 95% CI: 0.97-1.15; nine studies; 2787 women, low-certainty evidence); neonatal hypoglycemia (RR 0.93; 95% CI: 0.74-1.18; five studies; 880 women; low-certainty evidence); respiratory distress syndrome (RR 0.78; 95% CI: 0.47-1.29; four studies; 466 women; very low-certainty evidence); or shoulder dystocia (RR 0.28; 95% CI: 0.07-1.12; 2 studies; 530 women; very low-certainty evidence).
Conclusion: PCC for women with pre-gestational type 1 or type 2 diabetes mellitus is effective in improving rates of congenital malformations. In addition, it may improve the risk of preterm delivery and admission to NICU. PCC probably reduces maternal HbA1C in the first trimester of pregnancy, perinatal mortality and SGA. There is uncertainty regarding the effects of PCC on early booking for antenatal care or maternal hypoglycemia during the first trimester of pregnancy. PCC has little or no effect on other maternal and perinatal outcomes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- International Diabetes Federation. IDF Diabetes Atlas. 8th ed. Brussels, Belgium: IDF; [15 October 2019]. Available from: http://www.diabetesatlas.org.
-
- Temple R, Aldridge V, Greenwood R, Heyburn P, Sampson M, Stanley K. Association between outcome of pregnancy and glycaemic control in early pregnancy in type 1 diabetes: population based study. BMJ (Clinical research ed). 2002;325(7375):1275–6. Epub 2002/11/30. 10.1136/bmj.325.7375.1275 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
