

Low stroke incidence in the TEMPiS telestroke network during COVID-19 pandemic: Effect of lockdown on thrombolysis and thrombectomy
- PMID: 32811274
- PMCID: PMC7441481
- DOI: 10.1177/1357633X20943327
Low stroke incidence in the TEMPiS telestroke network during COVID-19 pandemic: Effect of lockdown on thrombolysis and thrombectomy
Abstract
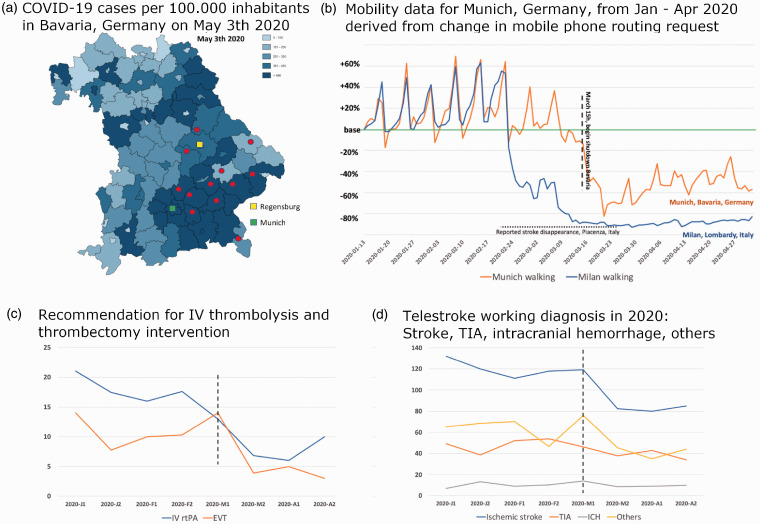
Background: During the COVID-19 pandemic emergency departments have noted a significant decrease in stroke patients. We performed a timely analysis of the Bavarian telestroke TEMPiS "working diagnosis" database.
Methods: Twelve hospitals from the TEMPiS network were selected. Data collected for January through April in years 2017 through 2020 were extracted and analyzed for presumed and definite ischemic stroke (IS), amongst other disorders. In addition, recommendations for intravenous thrombolysis (rtPA) and endovascular thrombectomy (EVT) were noted and mobility data of the region analyzed. If statistically valid, group-comparison was tested with Fisher's exact test considering unpaired observations and ap-value < 0.05 was considered significant.
Results: Upon lockdown in mid-March 2020, we observed a significant reduction in recommendations for rtPA compared to the preceding three years (14.7% [2017-2019] vs. 9.2% [2020], p = 0.0232). Recommendations for EVT were significantly higher in January to mid-March 2020 compared to 2017-2019 (5.4% [2017-2019] vs. 9.3% [2020], p = 0.0013) reflecting its increasing importance. Following the COVID-19 lockdown mid-March 2020 the number of EVT decreased back to levels in 2017-2019 (7.4% [2017-2019] vs. 7.6% [2020], p = 0.1719). Absolute numbers of IS decreased in parallel to mobility data.
Conclusions: The reduced stroke incidence during the COVID-19 pandemic may in part be explained by patient avoidance to seek emergency stroke care and may have an association to population mobility. Increasing mobility may induce a rebound effect and may conflict with a potential second COVID-19 wave. Telemedical networks may be ideal databases to study such effects in near-real time.
Keywords: COVID-19; Telestroke; lockdown; stroke; telehealth; thrombolysis.
Conflict of interest statement
Anonymized data are available on request.
Figures
References
-
- Jawaid A. Protecting older adults during social distancing. Science 2020; 368: 145. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
