

Cardiac Troponin I and Incident Stroke in European Cohorts: Insights From the BiomarCaRE Project
- PMID: 32811388
- PMCID: PMC7447179
- DOI: 10.1161/STROKEAHA.120.029452
Cardiac Troponin I and Incident Stroke in European Cohorts: Insights From the BiomarCaRE Project
Abstract
Background and purpose: Stroke is a common cause of death and a leading cause of disability and morbidity. Stroke risk assessment remains a challenge, but circulating biomarkers may improve risk prediction. Controversial evidence is available on the predictive ability of troponin concentrations and the risk of stroke in the community. Furthermore, reports on the predictive value of troponin concentrations for different stroke subtypes are scarce.
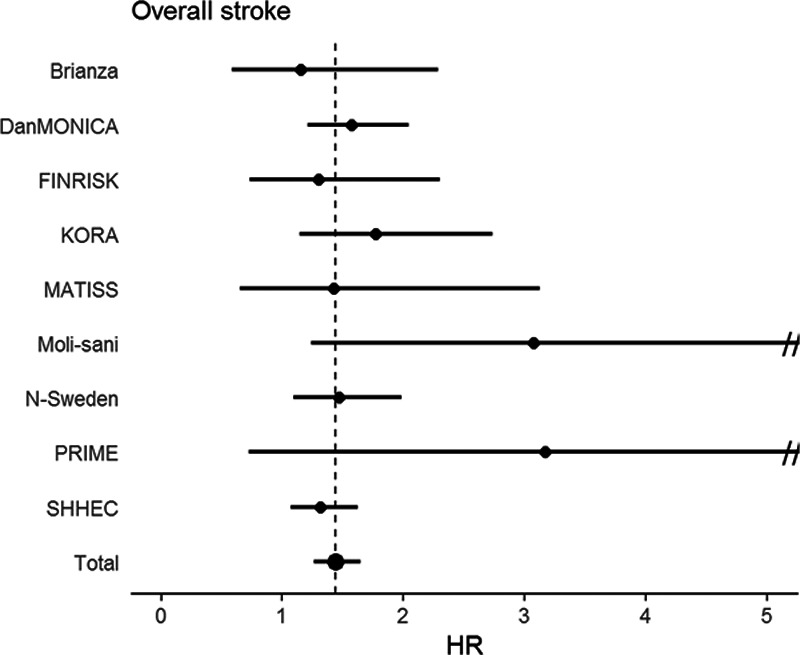
Methods: High-sensitivity cardiac troponin I (hsTnI) concentrations were assessed in 82 881 individuals (median age, 50.7 years; 49.7% men) free of stroke or myocardial infarction at baseline from 9 prospective European community cohorts. We used Cox proportional hazards regression to determine relative risks, followed by measures of discrimination and reclassification using 10-fold cross-validation to control for overoptimism. Follow-up was based upon linkage with national hospitalization registries and causes of death registries.
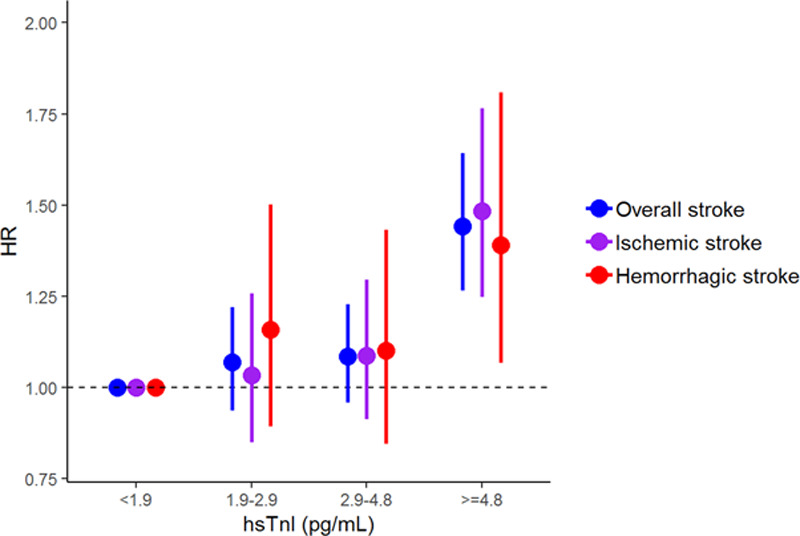
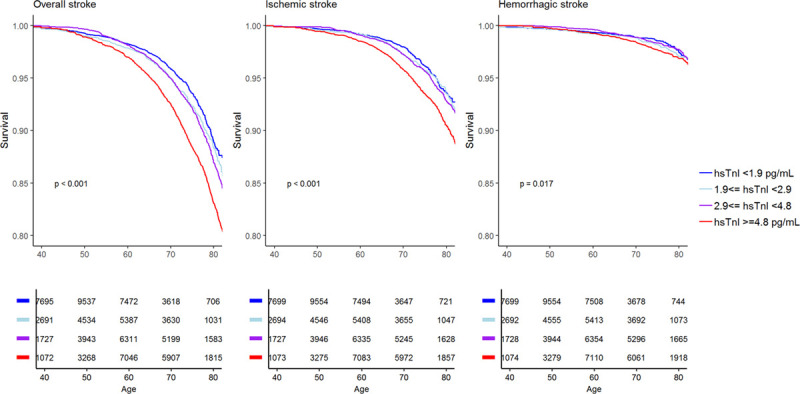
Results: Over a median follow-up of 12.7 years, 3033 individuals were diagnosed with incident nonfatal or fatal stroke (n=1654 ischemic strokes, n=612 hemorrhagic strokes, and n=767 indeterminate strokes). In multivariable regression models, hsTnI concentrations were associated with overall stroke (hazard ratio per 1-SD increase, 1.15 [95% CI, 1.10-1.21]), ischemic stroke (hazard ratio, 1.14 [95% CI, 1.09-1.21]), and hemorrhagic stroke (hazard ratio, 1.10 [95% CI, 1.01-1.20]). Adding hsTnI concentrations to classical cardiovascular risk factors (C indices, 0.809, 0.840, and 0.736 for overall, ischemic, and hemorrhagic stroke, respectively) increased the C index significantly but modestly. In individuals with an intermediate 10-year risk (5%-20%), the net reclassification improvement for overall stroke was 0.038 (P=0.021).
Conclusions: Elevated hsTnI concentrations are associated with an increased risk of incident stroke in the community, irrespective of stroke subtype. Adding hsTnI concentrations to classical risk factors only modestly improved estimation of 10-year risk of stroke in the overall cohort but might be of some value in individuals at an intermediate risk.
Keywords: cohort studies; epidemiology; risk assessment; stroke; troponin.
Conflict of interest statement
Dr Di Castelnuovo reports grants from the European Foundation for Alcohol Research as the coapplicant of the ongoing study supported by a research grant (id. EA1767) unrelated to the current study. Dr Kee reports funding from grants of the UK Clinical Research Collaboration and from the Wellcome Trust unrelated to the current work. Dr Schnabel reports personal fees from BMS/Pfizer and lecture and advisory board fees unrelated to the current study. Dr Blankenberg reports research funding from Abbott Diagnostics, Bayer, SIEMENS, Singulex, and Thermo Fisher. He further received honoraria for lectures from Abbott, Abbott Diagnostics, AstraZeneca, Bayer, AMGEN, Medtronic, Pfizer, Roche, SIEMENS Diagnostics, SIEMENS, and Thermo Fisher and as member of Advisory Boards and for consulting for Bayer, Novartis, and Thermo Fisher. Dr Costanzo reports funding from an ERAB grant (id. EA1767) and personal fees as a member of the Organizing Committee and speaker for the Ninth European Beer and Health Symposium (Bruxelles 2019) and for given lecture at the 13th European Nutrition Conference (FENS 2019, Dublin), all unrelated to the current work. Dr Söderberg reports personal fees from Actelion, Ltd. Dr Salomaa has received honoraria from Novo Nordisk and Sanofi for consultations. He also has ongoing research collaboration with Bayer AG (all unrelated to the present study). Dr Koenig reports personal fees from AstraZeneca, Novartis, Pfizer, The Medicines Company, DalCor, Kowa, Amgen, Corvidia, Berlin-Chemie, Sanofi, Bristol-Myers Squibb, and Daichii-Sankyo and nonfinancial support by grants from Abbott, Roche Diagnostics, Beckmann, and Singulex, all unrelated to the current study. The other authors report no conflicts.
Figures
References
-
- Meschia JF, Bushnell C, Boden-Albala B, Braun LT, Bravata DM, Chaturvedi S, Creager MA, Eckel RH, Elkind MS, Fornage M, et al. ; American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Functional Genomics and Translational Biology; Council on Hypertension Guidelines for the primary prevention of stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014453754–3832doi: 10.1161/STR.0000000000000046 - PMC - PubMed
-
- Adams JE, III, Bodor GS, Dávila-Román VG, Delmez JA, Apple FS, Ladenson JH, Jaffe AS. Cardiac troponin I. A marker with high specificity for cardiac injury. Circulation 199388101–106doi: 10.1161/01.cir.88.1.101 - PubMed
-
- Keller T, Zeller T, Peetz D, Tzikas S, Roth A, Czyz E, Bickel C, Baldus S, Warnholtz A, Fröhlich M, et al. Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med 2009361868–877doi: 10.1056/NEJMoa0903515 - PubMed
-
- Willeit P, Welsh P, Evans JDW, Tschiderer L, Boachie C, Jukema JW, Ford I, Trompet S, Stott DJ, Kearney PM, et al. High-sensitivity cardiac troponin concentration and risk of first-ever cardiovascular outcomes in 154,052 participants. J Am Coll Cardiol 201770558–568doi: 10.1016/j.jacc.2017.05.062 - PMC - PubMed
-
- Jia X, Sun W, Hoogeveen RC, Nambi V, Matsushita K, Folsom AR, Heiss G, Couper DJ, Solomon SD, Boerwinkle E, et al. High-sensitivity troponin I and incident coronary events, stroke, heart failure hospitalization, and mortality in the ARIC Study. Circulation 20191392642–2653doi: 10.1161/CIRCULATIONAHA.118.038772 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
