

Cross-Talk Between Key Players in Patients with COVID-19 and Ischemic Stroke: A Review on Neurobiological Insight of the Pandemic
- PMID: 32813238
- PMCID: PMC7434850
- DOI: 10.1007/s12035-020-02072-4
Cross-Talk Between Key Players in Patients with COVID-19 and Ischemic Stroke: A Review on Neurobiological Insight of the Pandemic
Abstract
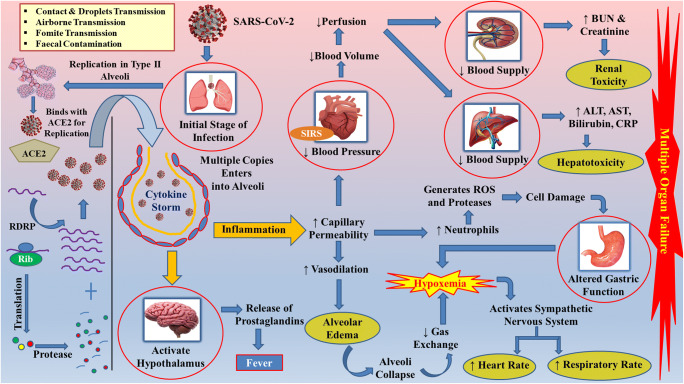
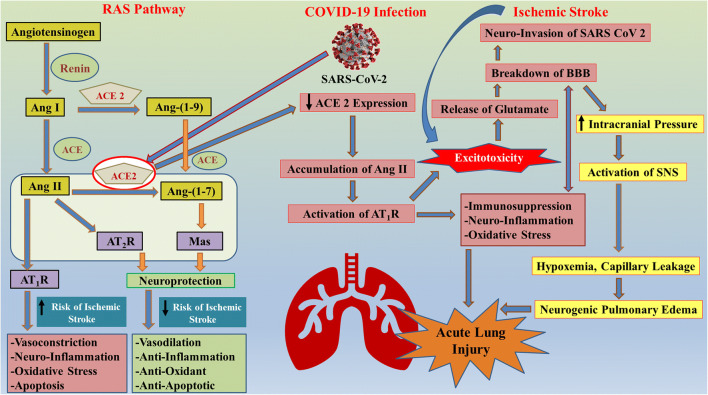
The global pandemic of novel coronavirus disease 2019 (COVID-19) has taken the entire human race by surprise and led to an unprecedented number of mortalities worldwide so far. Current clinical studies have interpreted that angiotensin-converting enzyme 2 (ACE2) is the host receptor for severe acute respiratory syndrome-coronavirus 2 (SARS-CoV-2). In addition, ACE2 is the major component of the renin-angiotensin system. ACE2 deteriorates angiotensin II, a peptide that is responsible for the promotion of stroke. The downregulation of ACE2 further activates an immunological cascade. Thus, researchers need to explore and examine the possible links between COVID-19 and ischemic stroke (IS). Human ACE2 expression level and pattern in various tissues might be decisive for the vulnerability, symptoms, and treatment outcomes of the SARS-CoV-2 infection. The swift increase in the knowledge of SARS-CoV-2 has given creditable evidence that SARS-CoV-2 infected patients also encounter neurological deficits. As the SARS-CoV-2 binds to ACE2, it will hamper the activity of ACE2 in providing neuroprotection, especially in the case of stroke patients. Due to the downregulation of ACE2, the inflammatory response is activated in the ischemic penumbra. The COVID-19 pandemic has affected people with various pre-existing diseases, including IS, in such a way that these patients need special care and attention for their survival. Several clinical trials are currently ongoing worldwide as well as many other projects are in different stages of conceptualization and planning to facilitate the effective management of stroke patients with COVID-19 infection.
Keywords: Angiotensin-converting enzyme 2; COVID-19; Inflammatory response; Ischemic stroke; Renin-angiotensin system.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Angiotensin-Converting Enzyme 2: SARS-CoV-2 Receptor and Regulator of the Renin-Angiotensin System: Celebrating the 20th Anniversary of the Discovery of ACE2.Circ Res. 2020 May 8;126(10):1456-1474. doi: 10.1161/CIRCRESAHA.120.317015. Epub 2020 Apr 8. Circ Res. 2020. PMID: 32264791 Free PMC article. Review.
-
Coronavirus Disease 2019 and Stroke: Clinical Manifestations and Pathophysiological Insights.J Stroke Cerebrovasc Dis. 2020 Aug;29(8):104941. doi: 10.1016/j.jstrokecerebrovasdis.2020.104941. Epub 2020 May 12. J Stroke Cerebrovasc Dis. 2020. PMID: 32689643 Free PMC article. Review.
-
Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19).J Pathol. 2020 Jul;251(3):228-248. doi: 10.1002/path.5471. Epub 2020 Jun 10. J Pathol. 2020. PMID: 32418199 Free PMC article. Review.
-
Renin-Angiotensin System Blockers and the COVID-19 Pandemic: At Present There Is No Evidence to Abandon Renin-Angiotensin System Blockers.Hypertension. 2020 Jun;75(6):1382-1385. doi: 10.1161/HYPERTENSIONAHA.120.15082. Epub 2020 Mar 25. Hypertension. 2020. PMID: 32208987 Free PMC article.
-
Spironolactone may provide protection from SARS-CoV-2: Targeting androgens, angiotensin converting enzyme 2 (ACE2), and renin-angiotensin-aldosterone system (RAAS).Med Hypotheses. 2020 Oct;143:110112. doi: 10.1016/j.mehy.2020.110112. Epub 2020 Jul 16. Med Hypotheses. 2020. PMID: 32721806 Free PMC article.
Cited by
-
Brain Arteriovenous Malformation Hemorrhage and Pituitary Adenoma in a COVID-19-Positive Patient.Cureus. 2024 Aug 23;16(8):e67644. doi: 10.7759/cureus.67644. eCollection 2024 Aug. Cureus. 2024. PMID: 39314610 Free PMC article.
-
Predicting COVID-19-Comorbidity Pathway Crosstalk-Based Targets and Drugs: Towards Personalized COVID-19 Management.Biomedicines. 2021 May 17;9(5):556. doi: 10.3390/biomedicines9050556. Biomedicines. 2021. PMID: 34067609 Free PMC article.
-
Incidence and predictors of organ failure among COVID-19 hospitalized adult patients in Eastern Ethiopia. Hospital-based retrospective cohort study.BMC Infect Dis. 2022 Apr 28;22(1):412. doi: 10.1186/s12879-022-07402-6. BMC Infect Dis. 2022. PMID: 35484484 Free PMC article.
-
Role of the renin-angiotensin system in the development of COVID-19-associated neurological manifestations.Front Cell Neurosci. 2022 Sep 16;16:977039. doi: 10.3389/fncel.2022.977039. eCollection 2022. Front Cell Neurosci. 2022. PMID: 36187294 Free PMC article. Review.
-
Unhealthy Dieting During the COVID-19 Pandemic: An Opinion Regarding the Harmful Effects on Brain Health.Front Nutr. 2022 Apr 28;9:876112. doi: 10.3389/fnut.2022.876112. eCollection 2022. Front Nutr. 2022. PMID: 35571935 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
