

Effects of Diet versus Gastric Bypass on Metabolic Function in Diabetes
- PMID: 32813948
- PMCID: PMC7456610
- DOI: 10.1056/NEJMoa2003697
Effects of Diet versus Gastric Bypass on Metabolic Function in Diabetes
Abstract
Background: Some studies have suggested that in people with type 2 diabetes, Roux-en-Y gastric bypass has therapeutic effects on metabolic function that are independent of weight loss.
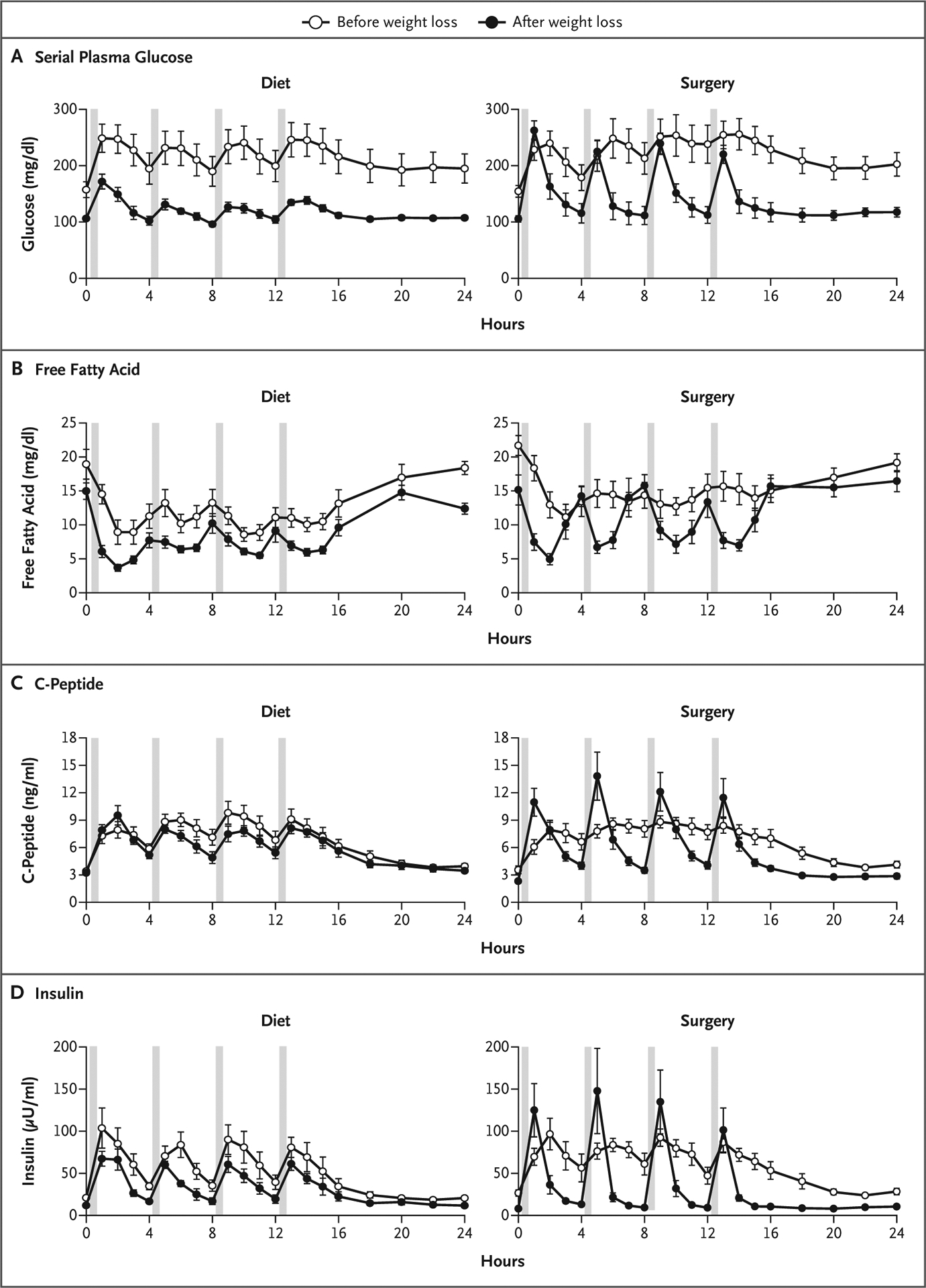
Methods: We evaluated metabolic regulators of glucose homeostasis before and after matched (approximately 18%) weight loss induced by gastric bypass (surgery group) or diet alone (diet group) in 22 patients with obesity and diabetes. The primary outcome was the change in hepatic insulin sensitivity, assessed by infusion of insulin at low rates (stages 1 and 2 of a 3-stage hyperinsulinemic euglycemic pancreatic clamp). Secondary outcomes were changes in muscle insulin sensitivity, beta-cell function, and 24-hour plasma glucose and insulin profiles.
Results: Weight loss was associated with increases in mean suppression of glucose production from baseline, by 7.04 μmol per kilogram of fat-free mass per minute (95% confidence interval [CI], 4.74 to 9.33) in the diet group and by 7.02 μmol per kilogram of fat-free mass per minute (95% CI, 3.21 to 10.84) in the surgery group during clamp stage 1, and by 5.39 (95% CI, 2.44 to 8.34) and 5.37 (95% CI, 2.41 to 8.33) μmol per kilogram of fat-free mass per minute in the two groups, respectively, during clamp stage 2; there were no significant differences between the groups. Weight loss was associated with increased insulin-stimulated glucose disposal, from 30.5±15.9 to 61.6±13.0 μmol per kilogram of fat-free mass per minute in the diet group and from 29.4±12.6 to 54.5±10.4 μmol per kilogram of fat-free mass per minute in the surgery group; there was no significant difference between the groups. Weight loss increased beta-cell function (insulin secretion relative to insulin sensitivity) by 1.83 units (95% CI, 1.22 to 2.44) in the diet group and by 1.11 units (95% CI, 0.08 to 2.15) in the surgery group, with no significant difference between the groups, and it decreased the areas under the curve for 24-hour plasma glucose and insulin levels in both groups, with no significant difference between the groups. No major complications occurred in either group.
Conclusions: In this study involving patients with obesity and type 2 diabetes, the metabolic benefits of gastric bypass surgery and diet were similar and were apparently related to weight loss itself, with no evident clinically important effects independent of weight loss. (Funded by the National Institutes of Health and others; ClinicalTrials.gov number, NCT02207777.).
Copyright © 2020 Massachusetts Medical Society.
Figures

Comment in
-
Bariatric Surgery and Restoration of Insulin Sensitivity - It's Weight Loss.N Engl J Med. 2020 Aug 20;383(8):777-778. doi: 10.1056/NEJMe2024212. N Engl J Med. 2020. PMID: 32813956 No abstract available.
-
Weight loss is the major player in bariatric surgery benefits.Nat Med. 2020 Nov;26(11):1678-1679. doi: 10.1038/s41591-020-1117-8. Nat Med. 2020. PMID: 33060852 No abstract available.
-
Effect of Diet versus Gastric Bypass on Metabolic Function in Diabetes.N Engl J Med. 2020 Dec 10;383(24):2390-2391. doi: 10.1056/NEJMc2030030. N Engl J Med. 2020. PMID: 33296568 No abstract available.
-
Effect of Diet versus Gastric Bypass on Metabolic Function in Diabetes.N Engl J Med. 2020 Dec 10;383(24):2391. doi: 10.1056/NEJMc2030030. N Engl J Med. 2020. PMID: 33296569 No abstract available.
-
Effect of Diet versus Gastric Bypass on Metabolic Function in Diabetes.N Engl J Med. 2020 Dec 10;383(24):2391-2392. doi: 10.1056/NEJMc2030030. N Engl J Med. 2020. PMID: 33296570 No abstract available.
-
Effect of Diet versus Gastric Bypass on Metabolic Function in Diabetes.N Engl J Med. 2020 Dec 10;383(24):2392-2393. doi: 10.1056/NEJMc2030030. N Engl J Med. 2020. PMID: 33296571 No abstract available.
-
Metabolischer Effekt der Adipositas-Op.?MMW Fortschr Med. 2021 Mar;163(4):26-27. doi: 10.1007/s15006-021-9687-z. MMW Fortschr Med. 2021. PMID: 33638832 Review. German. No abstract available.
References
-
- Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric-metabolic surgery versus conventional medical treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, single-centre, randomised controlled trial. Lancet 2015; 386: 964–73. - PubMed
-
- Dixon JB, O’Brien PE, Playfair J, et al. Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA 2008; 299: 316–23. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- R01 DK101578/DK/NIDDK NIH HHS/United States
- T32 HL130357/HL/NHLBI NIH HHS/United States
- R01ES027595/ES/NIEHS NIH HHS/United States
- P30 DK056341/DK/NIDDK NIH HHS/United States
- S10 OD020025/OD/NIH HHS/United States
- T32HL130357/HL/NHLBI NIH HHS/United States
- P30 DK063491/DK/NIDDK NIH HHS/United States
- U24DK097153/DK/NIDDK NIH HHS/United States
- P30DK063491/DK/NIDDK NIH HHS/United States
- K01DK116917/DK/NIDDK NIH HHS/United States
- P30 DK020579/DK/NIDDK NIH HHS/United States
- T32 DK007296/DK/NIDDK NIH HHS/United States
- U24 DK097153/DK/NIDDK NIH HHS/United States
- K01 DK116917/DK/NIDDK NIH HHS/United States
- R01 ES027595/ES/NIEHS NIH HHS/United States
- R01DK101578/DK/NIDDK NIH HHS/United States
- P42ES010337/ES/NIEHS NIH HHS/United States
- P42 ES010337/ES/NIEHS NIH HHS/United States
- P30DK56341/DK/NIDDK NIH HHS/United States
- T32DK007296/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials