

Compassionate use of JAK1/2 inhibitor ruxolitinib for severe COVID-19: a prospective observational study
- PMID: 32814839
- PMCID: PMC7437386
- DOI: 10.1038/s41375-020-01018-y
Compassionate use of JAK1/2 inhibitor ruxolitinib for severe COVID-19: a prospective observational study
Abstract
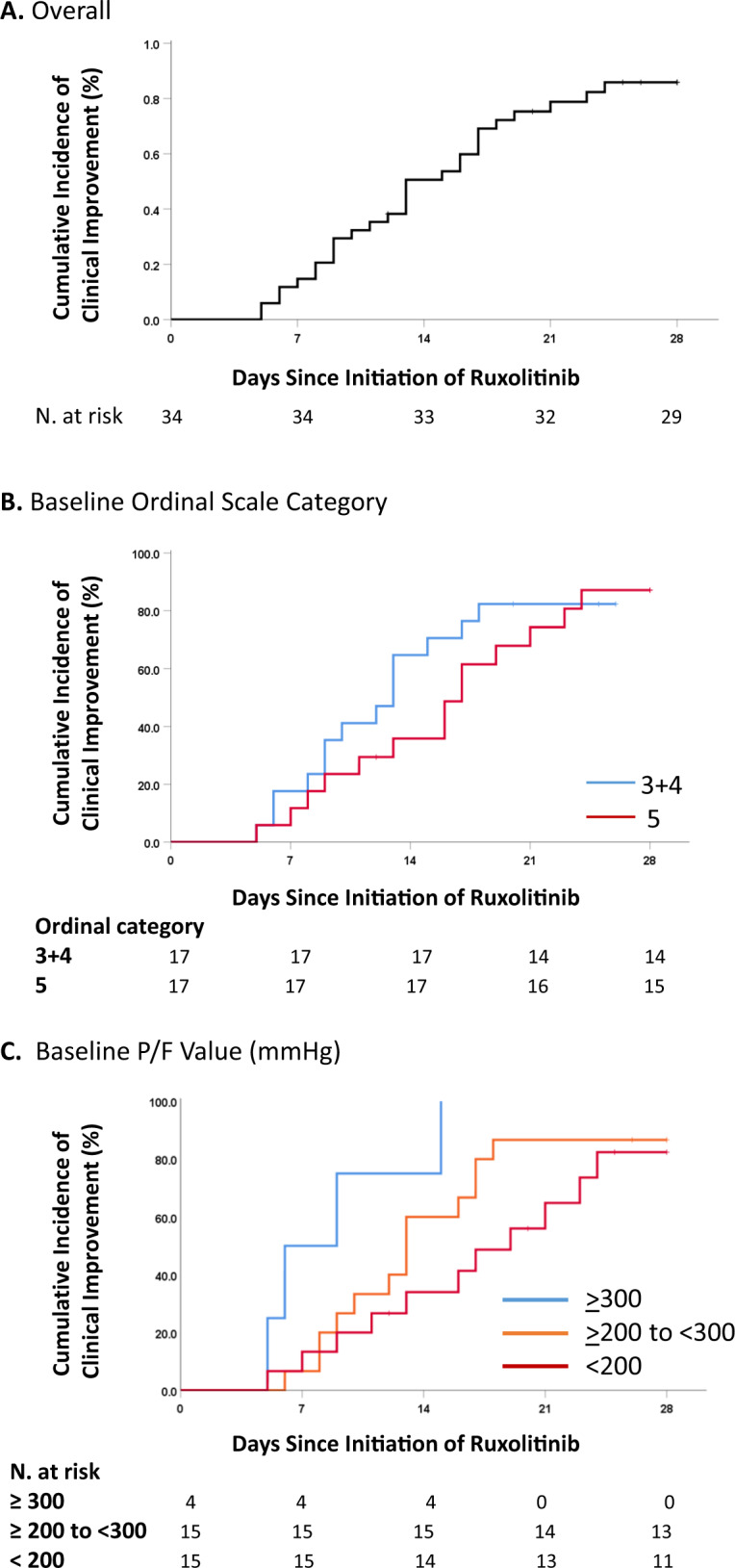
Overwhelming inflammatory reactions contribute to respiratory distress in patients with COVID-19. Ruxolitinib is a JAK1/JAK2 inhibitor with potent anti-inflammatory properties. We report on a prospective, observational study in 34 patients with COVID-19 who received ruxolitinib on a compassionate-use protocol. Patients had severe pulmonary disease defined by pulmonary infiltrates on imaging and an oxygen saturation ≤ 93% in air and/or PaO2/FiO2 ratio ≤ 300 mmHg. Median age was 80.5 years, and 85.3% had ≥ 2 comorbidities. Median exposure time to ruxolitinib was 13 days, median dose intensity was 20 mg/day. Overall survival by day 28 was 94.1%. Cumulative incidence of clinical improvement of ≥2 points in the ordinal scale was 82.4% (95% confidence interval, 71-93). Clinical improvement was not affected by low-flow versus high-flow oxygen support but was less frequent in patients with PaO2/FiO2 < 200 mmHg. The most frequent adverse events were anemia, urinary tract infections, and thrombocytopenia. Improvement of inflammatory cytokine profile and activated lymphocyte subsets was observed at day 14. In this prospective cohort of aged and high-risk comorbidity patients with severe COVID-19, compassionate-use ruxolitinib was safe and was associated with improvement of pulmonary function and discharge home in 85.3%. Controlled clinical trials are necessary to establish efficacy of ruxolitinib in COVID-19.
Conflict of interest statement
AMV has been in advisory board, and received fees for lectures, from Novartis. All other authors have no conflict of interest to report.
Figures



References
-
- Paules CI, Marston HD, Fauci AS. Coronavirus infections-more than just the common cold. JAMA. 2020. 10.1001/jama.2020.0757. - PubMed
-
- Centers for Disease Control and Prevention. Severe outcomes among patients with Coronavirus disease 2019 (COVID‐19)—United States. https://www.cdc.gov/mmwr/volumes/69/wr/mm6912e2.htm (2020).
-
- Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, et al. Remdesivir for the treatment of Covid-19—preliminary report. N Engl J Med. 2020; 10.1056/NEJMoa2007764. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
