

Risks and features of secondary infections in severe and critical ill COVID-19 patients
- PMID: 32815458
- PMCID: PMC8284966
- DOI: 10.1080/22221751.2020.1812437
Risks and features of secondary infections in severe and critical ill COVID-19 patients
Abstract
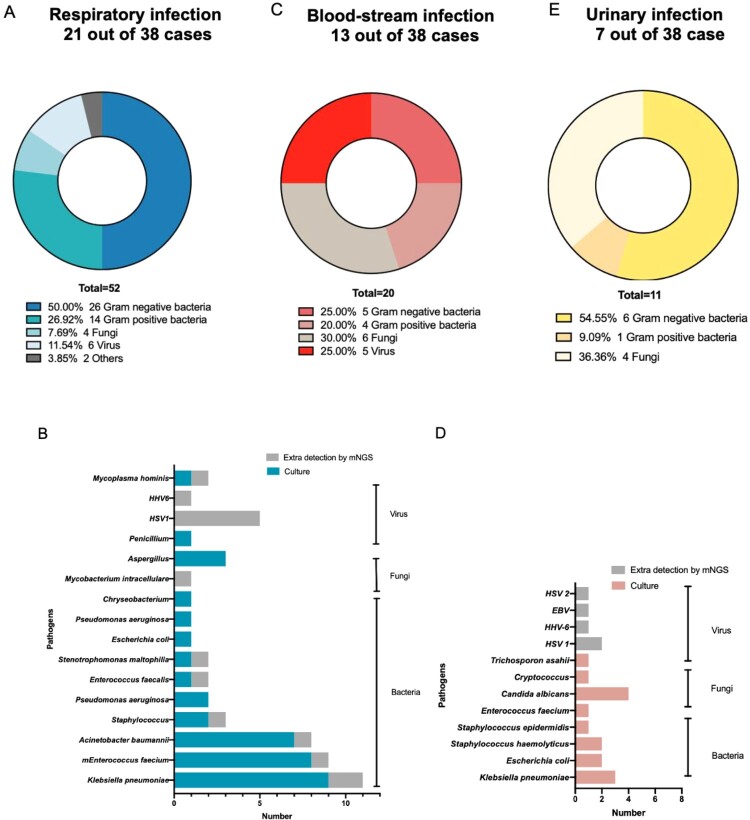
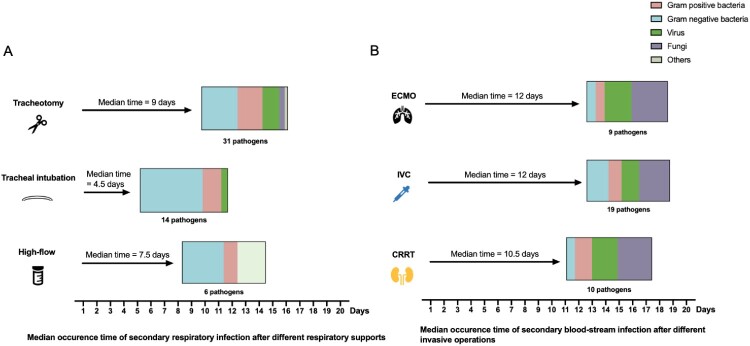
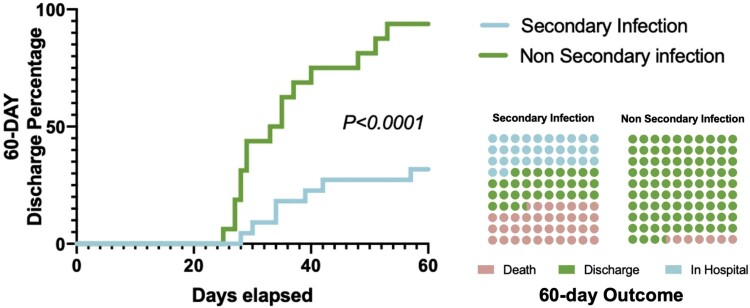
Objectives Severe or critical COVID-19 is associated with intensive care unit admission, increased secondary infection rate, and would lead to significant worsened prognosis. Risks and characteristics relating to secondary infections in severe COVID-19 have not been described. Methods Severe and critical COVID-19 patients from Shanghai were included. We collected lower respiratory, urine, catheters, and blood samples according to clinical necessity and culture and mNGS were performed. Clinical and laboratory data were archived. Results We found 57.89% (22/38) patients developed secondary infections. The patient receiving invasive mechanical ventilation or in critical state has a higher chance of secondary infections (P<0.0001). The most common infections were respiratory, blood-stream and urinary infections, and in respiratory infections, the most detected pathogens were gram-negative bacteria (26, 50.00%), following by gram-positive bacteria (14, 26.92%), virus (6, 11.54%), fungi (4, 7.69%), and others (2, 3.85%). Respiratory Infection rate post high flow, tracheal intubation, and tracheotomy were 12.90% (4/31), 30.43% (7/23), and 92.31% (12/13) respectively. Secondary infections would lead to lower discharge rate and higher mortality rate. Conclusion Our study originally illustrated secondary infection proportion in severe and critical COVID-19 patients. Culture accompanied with metagenomics sequencing increased pathogen diagnostic rate. Secondary infections risks increased after receiving invasive respiratory ventilations and intravascular devices, and would lead to a lower discharge rate and a higher mortality rate.
Keywords: COVID-19; SARS-CoV-2; intensive care; intravascular devices; respiratory ventilations; secondary infection.
Conflict of interest statement
All authors report no potential conflict of interest.
No potential conflict of interest was reported by the author(s).
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous