

Heterogeneous trends in burden of heart disease mortality by subtypes in the United States, 1999-2018: observational analysis of vital statistics
- PMID: 32816805
- PMCID: PMC7424397
- DOI: 10.1136/bmj.m2688
Heterogeneous trends in burden of heart disease mortality by subtypes in the United States, 1999-2018: observational analysis of vital statistics
Erratum in
-
Heterogeneous trends in burden of heart disease mortality by subtypes in the United States, 1999-2018: observational analysis of vital statistics.BMJ. 2020 Sep 3;370:m3380. doi: 10.1136/bmj.m3380. BMJ. 2020. PMID: 32883698 Free PMC article. No abstract available.
Abstract
Objective: To describe trends in the burden of mortality due to subtypes of heart disease from 1999 to 2018 to inform targeted prevention strategies and reduce disparities.
Design: Serial cross sectional analysis of cause specific heart disease mortality rates using national death certificate data in the overall population as well as stratified by race-sex, age, and geography.
Setting: United States, 1999-2018.
Participants: 12.9 million decedents from total heart disease (49% women, 12% black, and 19% <65 years old).
Main outcome measures: Age adjusted mortality rates (AAMR) and years of potential life lost (YPLL) for each heart disease subtype, and respective mean annual percentage change.
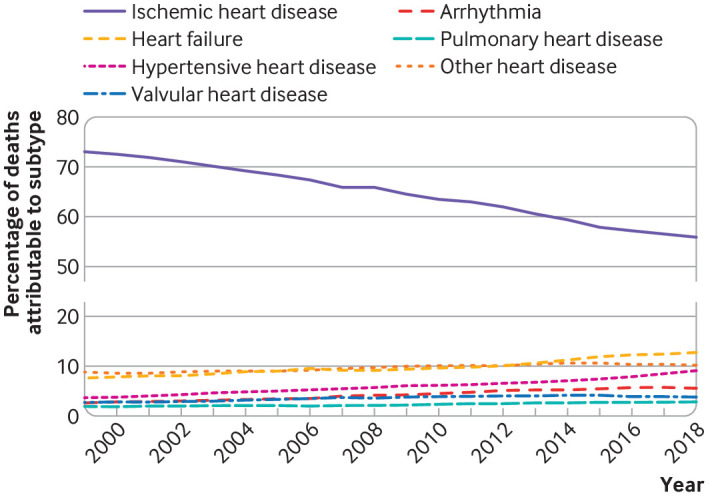
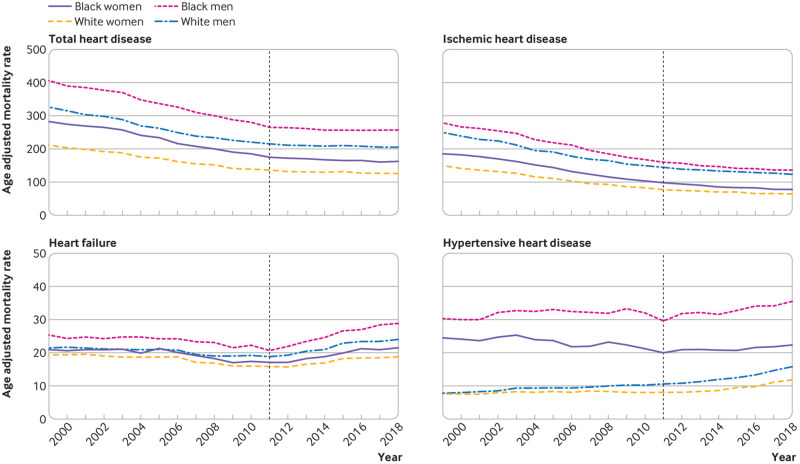
Results: Deaths from total heart disease fell from 752 192 to 596 577 between 1999 and 2011, and then increased to 655 381 in 2018. From 1999 to 2018, the proportion of total deaths from heart disease attributed to ischemic heart disease decreased from 73% to 56%, while the proportion attributed to heart failure increased from 8% to 13% and the proportion attributed to hypertensive heart disease increased from 4% to 9%. Among heart disease subtypes, AAMR was consistently highest for ischemic heart disease in all subgroups (race-sex, age, and region). After 2011, AAMR for heart failure and hypertensive heart disease increased at a faster rate than for other subtypes. The fastest increases in heart failure mortality were in black men (mean annual percentage change 4.9%, 95% confidence interval 4.0% to 5.8%), whereas the fastest increases in hypertensive heart disease occurred in white men (6.3%, 4.9% to 9.4%). The burden of years of potential life lost was greatest from ischemic heart disease, but black-white disparities were driven by heart failure and hypertensive heart disease. Deaths from heart disease in 2018 resulted in approximately 3.8 million potential years of life lost.
Conclusions: Trends in AAMR and years of potential life lost for ischemic heart disease have decelerated since 2011. For almost all other subtypes of heart disease, AAMR and years of potential life lost became stagnant or increased. Heart failure and hypertensive heart disease account for the greatest increases in premature deaths and the largest black-white disparities and have offset declines in ischemic heart disease. Early and targeted primary and secondary prevention and control of risk factors for heart disease, with a focus on groups at high risk, are needed to avoid these suboptimal trends beginning earlier in life.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the NIH National Heart, Lung, and Blood Institute, the NIH National Center for Advancing Translational Sciences, and the American Heart Association for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Centers for Disease Control and Prevention (CDC) Decline in deaths from heart disease and stroke--United States, 1900-1999. MMWR Morb Mortal Wkly Rep 1999;48:649-56. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical