

Mycophenolate Mofetil in C3 Glomerulopathy and Pathogenic Drivers of the Disease
- PMID: 32816888
- PMCID: PMC7480558
- DOI: 10.2215/CJN.15241219
Mycophenolate Mofetil in C3 Glomerulopathy and Pathogenic Drivers of the Disease
Erratum in
-
Correction.Clin J Am Soc Nephrol. 2020 Dec 7;15(12):1817. doi: 10.2215/CJN.16691020. Epub 2020 Nov 9. Clin J Am Soc Nephrol. 2020. PMID: 33168634 Free PMC article. No abstract available.
Abstract
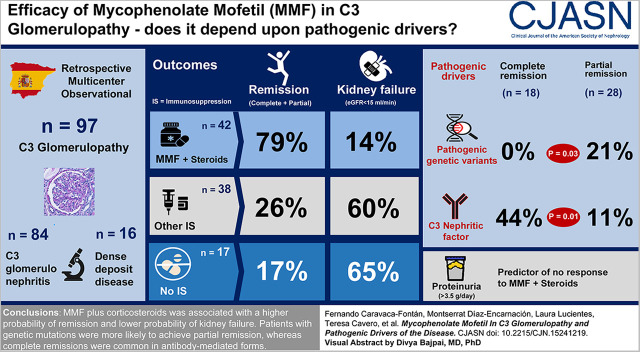
Background and objectives: C3 glomerulopathy is a complement-mediated disease arising from abnormalities in complement genes and/or antibodies against complement components. Previous studies showed that treatment with corticosteroids plus mycophenolate mofetil (MMF) was associated with improved outcomes, although the genetic profile of these patients was not systematically analyzed. This study aims to analyze the main determinants of disease progression and response to this therapeutic regimen.
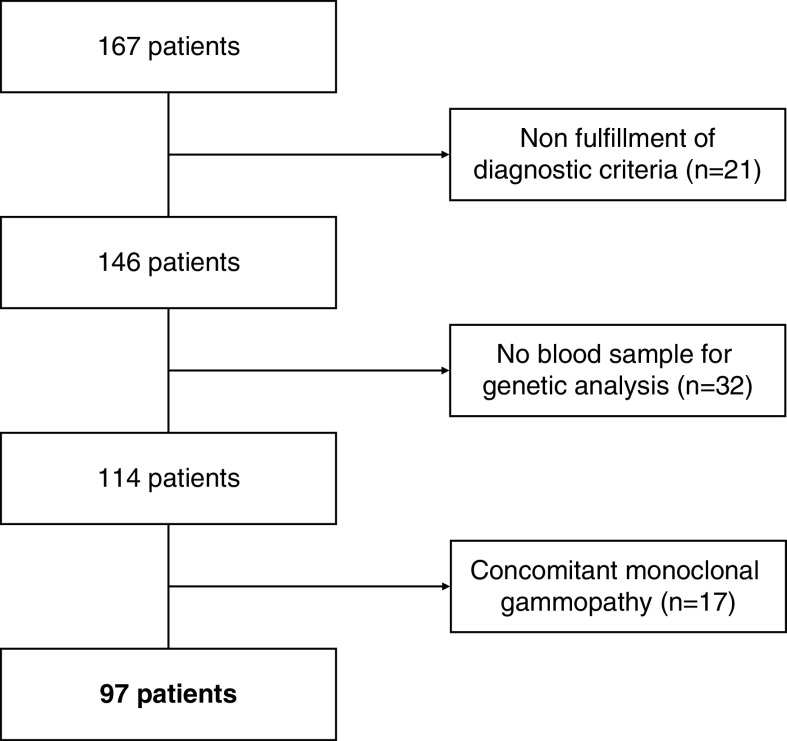
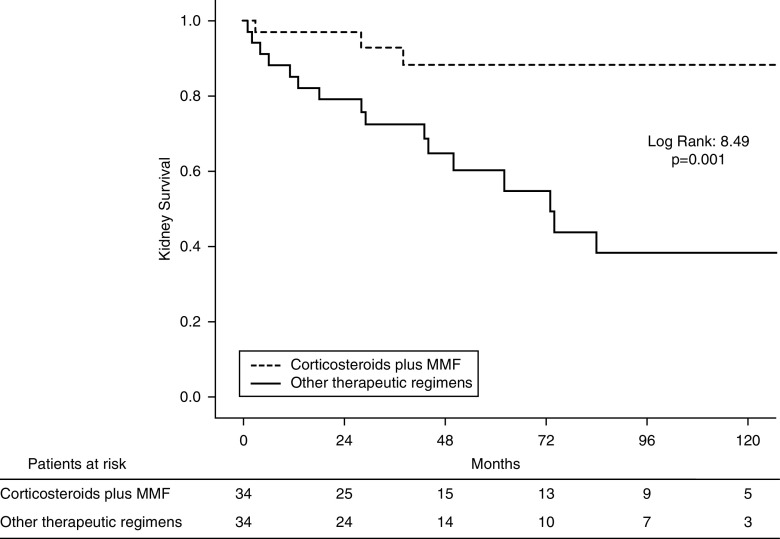
Design, setting, participants, & measurements: We conducted a retrospective, multicenter, observational cohort study in 35 nephrology departments belonging to the Spanish Group for the Study of Glomerular Diseases. Patients diagnosed with C3 glomerulopathy (n=81) or dense deposit disease (n=16) between January 1995 and March 2018 were enrolled. Multivariable and propensity score matching analyses were used to evaluate the association of clinical and genetic factors with response to treatment with corticosteroids and MMF as measured by proportion of patients with disease remission and kidney survival (status free of kidney failure).
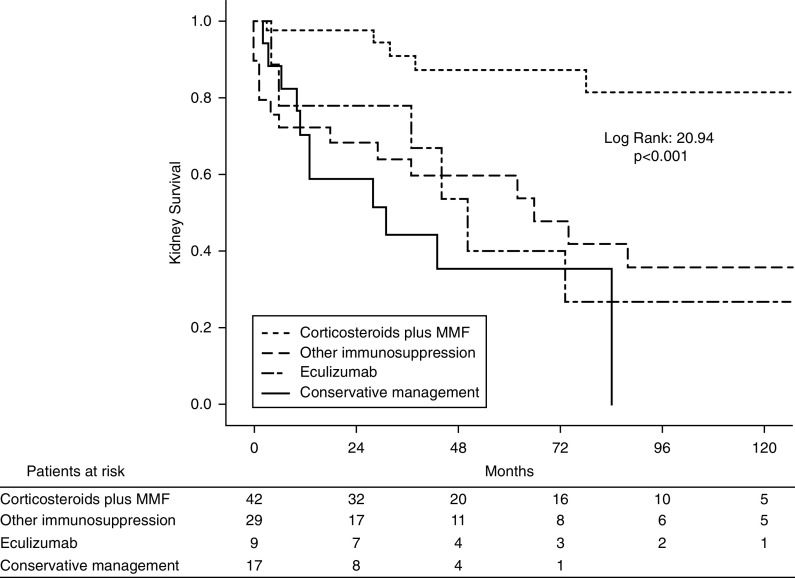
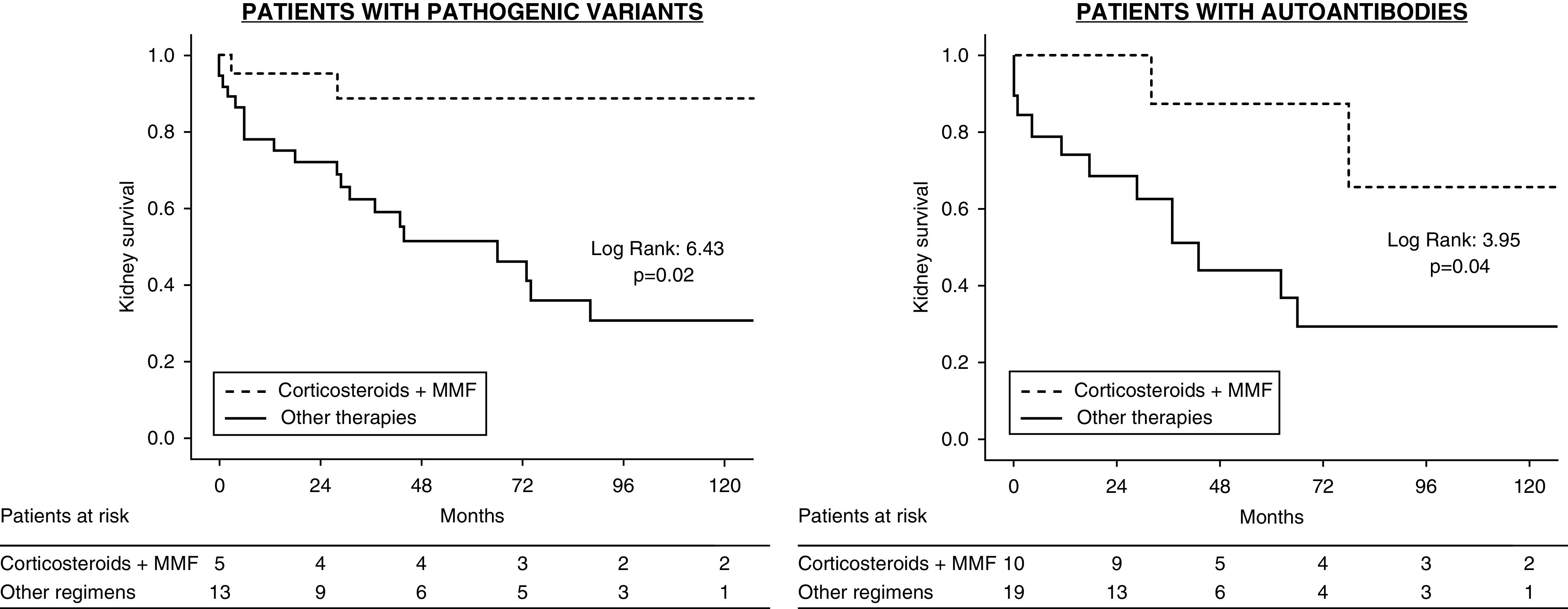
Results: The study group comprised 97 patients (84% C3 glomerulopathy, 16% dense deposit disease). Forty-two patients were treated with corticosteroids plus MMF, and this treatment was associated with a higher rate of remission and lower probability of kidney failure (79% and 14%, respectively) compared with patients treated with other immunosuppressives (24% and 59%, respectively), or ecluzimab (33% and 67%, respectively), or conservative management (18% and 65%, respectively). The therapeutic superiority of corticosteroids plus MMF was observed both in patients with complement abnormalities and with autoantibodies. However, patients with pathogenic variants in complement genes only achieved partial remission, whereas complete remissions were common among patients with autoantibody-mediated forms. The main determinant of no remission was baseline proteinuria. Relapses occurred after treatment discontinuation in 33% of the patients who had achieved remission with corticosteroids plus MMF, and a longer treatment length of MMF was associated with a lower risk of relapse.
Conclusions: The beneficial response to corticosteroids plus MMF treatment in C3 glomerulopathy appears independent of the pathogenic drivers analyzed in this study.
Keywords: Alternative complement pathway; C3 glomerulopathy; mycophenolate mofetil.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
Mycophenolate Mofetil Treatment of C3 Glomerulopathy.Clin J Am Soc Nephrol. 2020 Sep 7;15(9):1234-1236. doi: 10.2215/CJN.11740720. Epub 2020 Aug 19. Clin J Am Soc Nephrol. 2020. PMID: 32841154 Free PMC article. No abstract available.
References
-
- Smith RJH, Appel GB, Blom AM, Cook HT, D’Agati VD, Fakhouri F, Fremeaux-Bacchi V, Józsi M, Kavanagh D, Lambris JD, Noris M, Pickering MC, Remuzzi G, de Córdoba SR, Sethi S, Van der Vlag J, Zipfel PF, Nester CM: C3 glomerulopathy - understanding a rare complement-driven renal disease. Nat Rev Nephrol 15: 129–143, 2019. - PMC - PubMed
-
- Bomback AS, Appel GB: Pathogenesis of the C3 glomerulopathies and reclassification of MPGN. Nat Rev Nephrol 8: 634–642, 2012. - PubMed
-
- Cook HT: Evolving complexity of complement-related diseases: C3 glomerulopathy and atypical haemolytic uremic syndrome. Curr Opin Nephrol Hypertens 27: 165–170, 2018. - PubMed
-
- Zhao W, Ding Y, Lu J, Zhang T, Chen D, Zhang H, Zeng C, Liu Z, Chen H: Genetic analysis of the complement pathway in C3 glomerulopathy. Nephrol Dial Transplant 33: 1919–1927, 2018. - PubMed
-
- Iatropoulos P, Noris M, Mele C, Piras R, Valoti E, Bresin E, Curreri M, Mondo E, Zito A, Gamba S, Bettoni S, Murer L, Fremeaux-Bacchi V, Vivarelli M, Emma F, Daina E, Remuzzi G: Complement gene variants determine the risk of immunoglobulin-associated MPGN and C3 glomerulopathy and predict long-term renal outcome. Mol Immunol 71: 131–142, 2016. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
