

Efficacy and safety of adjunctive lacosamide in the treatment of primary generalised tonic-clonic seizures: a double-blind, randomised, placebo-controlled trial
- PMID: 32817358
- PMCID: PMC7509528
- DOI: 10.1136/jnnp-2020-323524
Efficacy and safety of adjunctive lacosamide in the treatment of primary generalised tonic-clonic seizures: a double-blind, randomised, placebo-controlled trial
Abstract
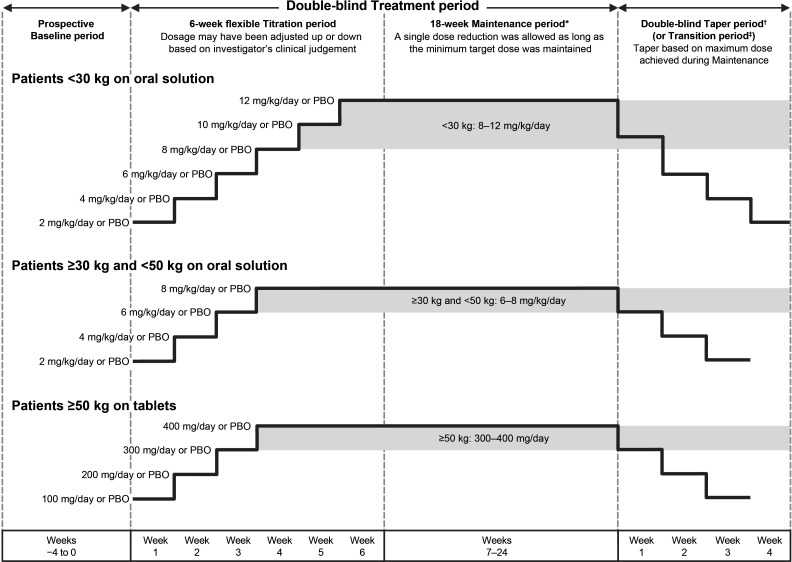
Objective: To evaluate efficacy and safety of lacosamide (up to 12 mg/kg/day or 400 mg/day) as adjunctive treatment for uncontrolled primary generalised tonic-clonic seizures (PGTCS) in patients (≥4 years) with idiopathic generalised epilepsy (IGE).
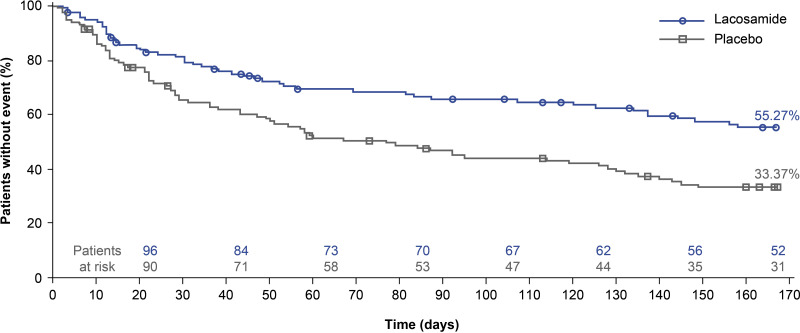
Methods: Phase 3, double-blind, randomised, placebo-controlled trial (SP0982; NCT02408523) in patients with IGE and PGTCS taking 1-3 concomitant antiepileptic drugs. Primary outcome was time to second PGTCS during 24-week treatment.
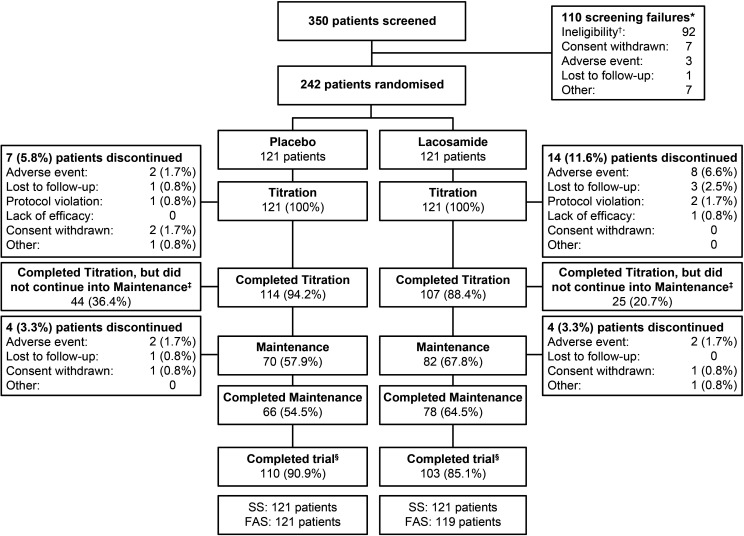
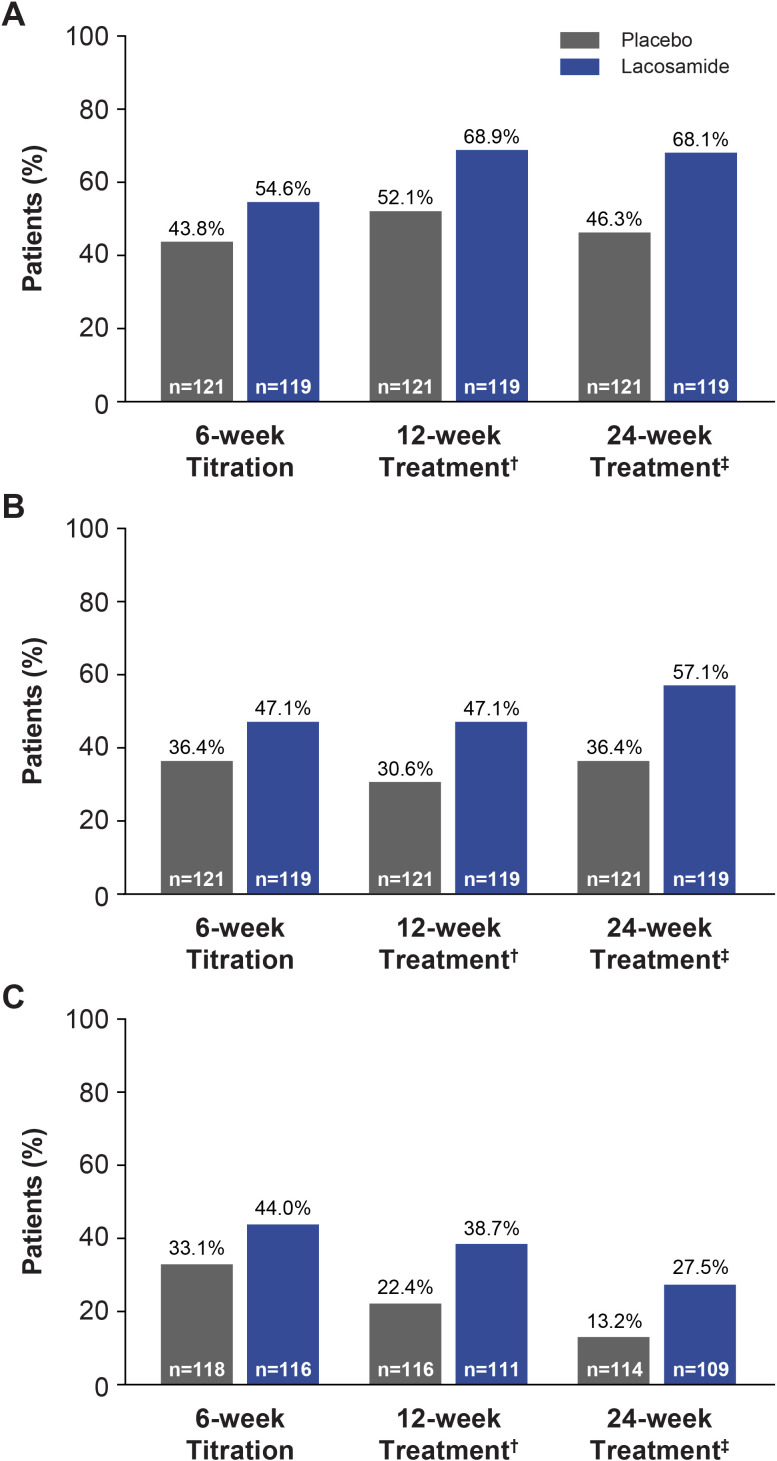
Results: 242 patients were randomised and received ≥1 dose of trial medication (lacosamide/placebo: n=121/n=121). Patients (mean age: 27.7 years; 58.7% female) had a history of generalised-onset seizures (tonic-clonic 99.6%; myoclonic 38.8%; absence 37.2%). Median treatment duration with lacosamide/placebo was 143/65 days. Risk of developing a second PGTCS during 24-week treatment was significantly lower with lacosamide than placebo (Kaplan-Meier survival estimates 55.27%/33.37%; HR 0.540, 95% CI 0.377 to 0.774; p<0.001; n=118/n=121). Median time to second PGTCS could not be estimated for lacosamide (>50% of patients did not experience a second PGTCS) and was 77.0 days for placebo. Kaplan-Meier estimated freedom from PGTCS at end of the 24-week treatment period (day 166) for lacosamide/placebo was 31.3%/17.2% (difference 14.1%; p=0.011). More patients on lacosamide than placebo had ≥50% (68.1%/46.3%) or ≥75% (57.1%/36.4%) reduction from baseline in PGTCS frequency/28 days, or observed freedom from PGTCS during treatment (27.5%/13.2%) (n=119/n=121). 96/121 (79.3%) patients on lacosamide had treatment-emergent adverse events (placebo 79/121 (65.3%)), most commonly dizziness (23.1%), somnolence (16.5%), headache (14.0%). No patients died during the trial.
Conclusions: Lacosamide was efficacious and generally safe as adjunctive treatment for uncontrolled PGTCS in patients with IGE.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DGV received speaker honoraria from Eisai, Greenwich Biosciences, Lundbeck, Sunovion and UCB Pharma; his institution received payments for his services as a principal investigator on randomised controlled trials sponsored by Biogen, Eisai, SK Life Science and UCB Pharma; he served as an advisor to Otsuka Pharmaceutical Development and Commercialisation and SK Life Science. SK received speaker honoraria from Desitin, Eisai and UCB Pharma. TJO received research funding from Anavex, Biogen, Eisai, Praxis Precision Medicines, UCB Pharma and Zynerba. MW received speaker honoraria from Eisai, Otsuka Pharmaceutical and UCB Pharma. MB, BS-B, PW and RR are employees of UCB Pharma.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources