

Establishment of age group classification for risk stratification in glioma patients
- PMID: 32819307
- PMCID: PMC7439690
- DOI: 10.1186/s12883-020-01888-w
Establishment of age group classification for risk stratification in glioma patients
Abstract
Background: Age is associated with the prognosis of glioma patients, but there is no uniform standard of age-group classification to evaluate the prognosis of glioma patients. In this study, we aimed to establish an age group classification for risk stratification in glioma patients.
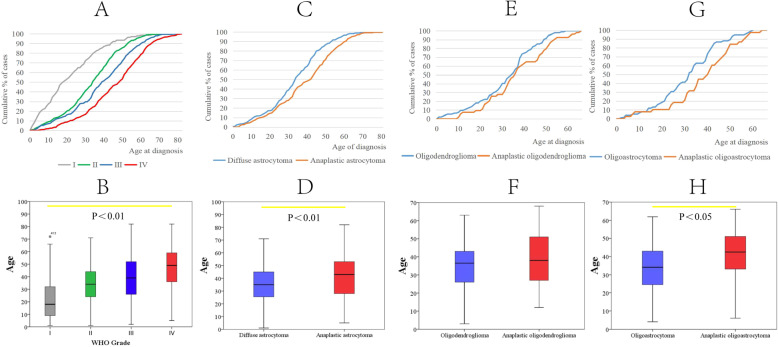
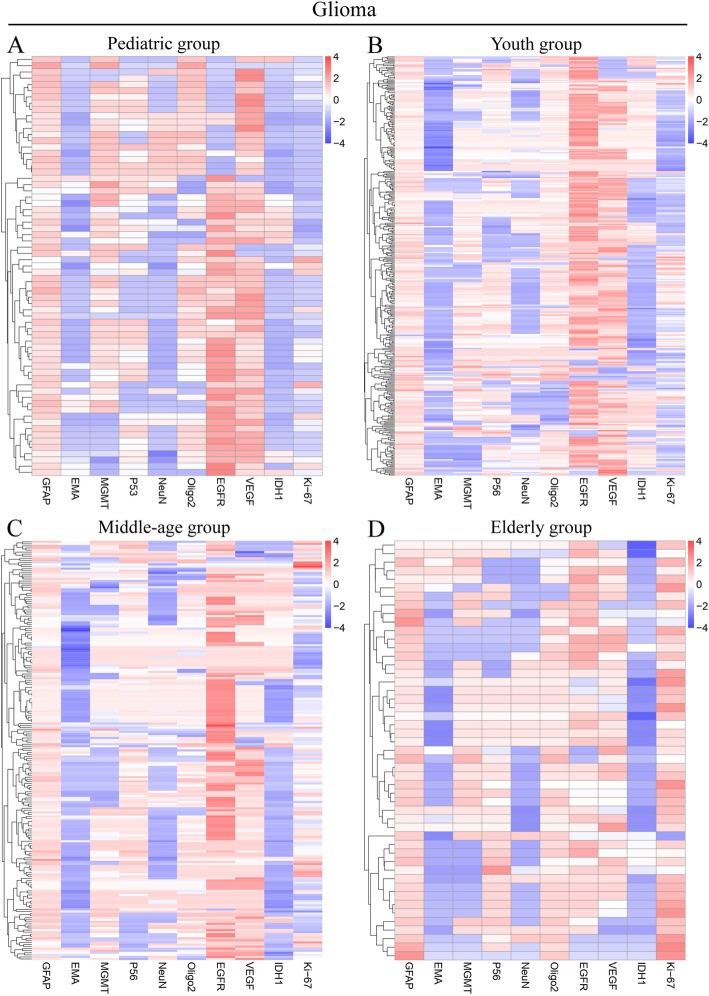
Methods: 1502 patients diagnosed with gliomas at Nanfang Hospital between 2000 and 2018 were enrolled. The WHO grade of glioma was used as a dependent variable to evaluate the effect of age on risk stratification. The evaluation model was established by logistic regression, and the Akaike information criterion (AIC) value of the model was used to determine the optimal cutoff points for age-classification. The differences in gender, WHO grade, pathological subtype, tumor cell differentiation, tumor size, tumor location, and molecular markers between different age groups were analyzed. The molecular markers included GFAP, EMA, MGMT, P53, NeuN, Oligo2, EGFR, VEGF, IDH1, Ki-67, PR, CD3, H3K27M, TS, and 1p/19q status.
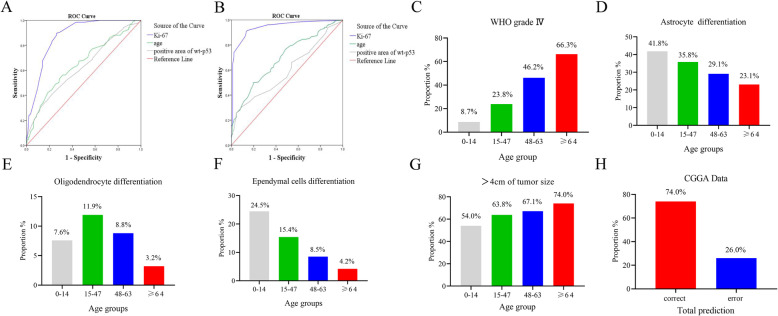
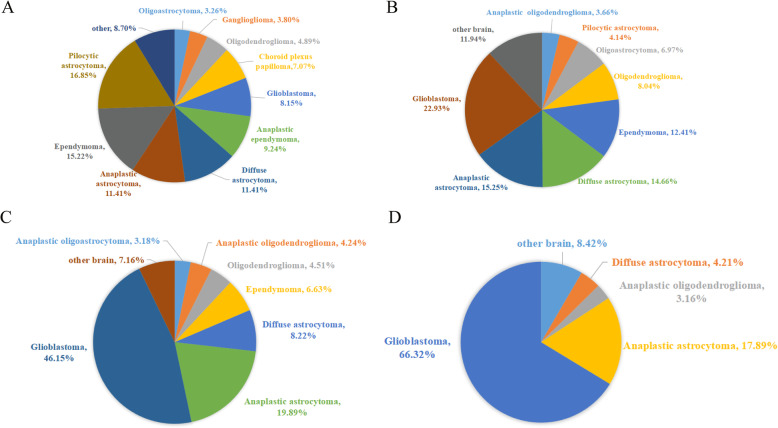
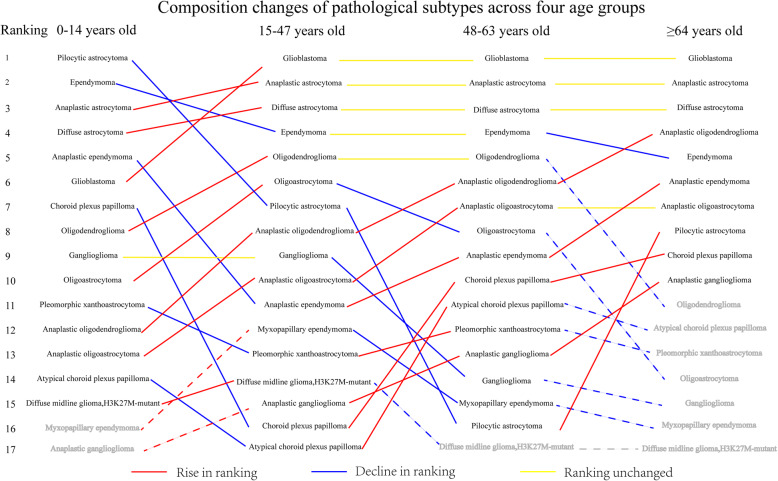
Results: The proportion of men with glioma was higher than that of women with glioma (58.3% vs 41.7%). Analysis of age showed that appropriate classifications of age group were 0-14 years old (pediatric group), 15-47 years old (youth group), 48-63 years old (middle-aged group), and ≥ 64 years old (elderly group).The proportions of glioblastoma and large tumor size (4-6 cm) increased with age (p = 0.000, p = 0.018, respectively). Analysis of the pathological molecular markers across the four age groups showed that the proportion of patients with larger than 10% area of Ki-67 expression or positive PR expression increased with age (p = 0.000, p = 0.017, respectively).
Conclusions: Appropriate classifications of the age group for risk stratification are 0-14 years old (pediatric group), 15-47 years old (young group), 48-63 years old (middle age group) and ≥ 64 years old (elderly group). This age group classification is effective in evaluating the risk of glioblastoma in glioma patients.
Keywords: Age group classification; Glioma; Personalized treatment; Risk stratification.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Usinskiene J, Ulyte A, Bjornerud A, Venius J, Katsaros VK, Rynkeviciene R, et al. Optimal differentiation of high- and low-grade glioma and metastasis: a meta-analysis of perfusion, diffusion, and spectroscopy metrics. Neuroradiology. 2016;58(4):339–350. doi: 10.1007/s00234-016-1642-9. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
