

Circulating tumor DNA guided adjuvant chemotherapy in stage II colon cancer (MEDOCC-CrEATE): study protocol for a trial within a cohort study
- PMID: 32819390
- PMCID: PMC7441668
- DOI: 10.1186/s12885-020-07252-y
Circulating tumor DNA guided adjuvant chemotherapy in stage II colon cancer (MEDOCC-CrEATE): study protocol for a trial within a cohort study
Abstract
Background: Accurate detection of patients with minimal residual disease (MRD) after surgery for stage II colon cancer (CC) remains an urgent unmet clinical need to improve selection of patients who might benefit form adjuvant chemotherapy (ACT). Presence of circulating tumor DNA (ctDNA) is indicative for MRD and has high predictive value for recurrent disease. The MEDOCC-CrEATE trial investigates how many stage II CC patients with detectable ctDNA after surgery will accept ACT and whether ACT reduces the risk of recurrence in these patients.
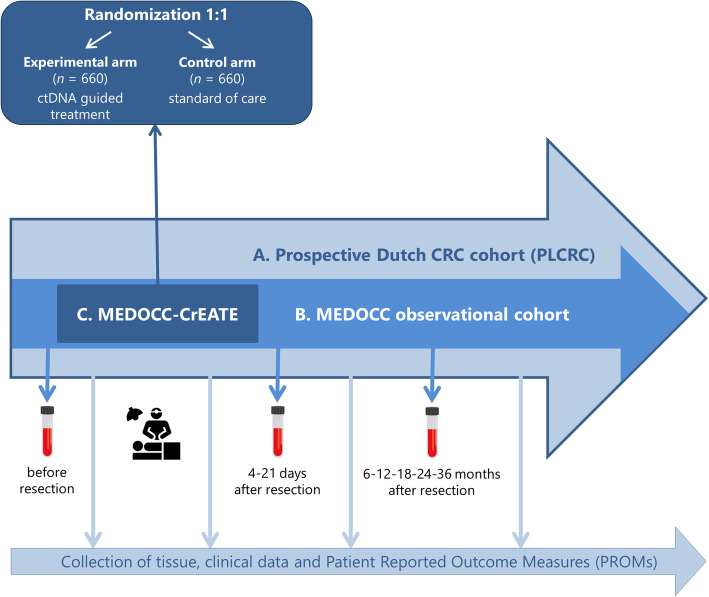
Methods/design: MEDOCC-CrEATE follows the 'trial within cohorts' (TwiCs) design. Patients with colorectal cancer (CRC) are included in the Prospective Dutch ColoRectal Cancer cohort (PLCRC) and give informed consent for collection of clinical data, tissue and blood samples, and consent for future randomization. MEDOCC-CrEATE is a subcohort within PLCRC consisting of 1320 stage II CC patients without indication for ACT according to current guidelines, who are randomized 1:1 into an experimental and a control arm. In the experimental arm, post-surgery blood samples and tissue are analyzed for tissue-informed detection of plasma ctDNA, using the PGDx elio™ platform. Patients with detectable ctDNA will be offered ACT consisting of 8 cycles of capecitabine plus oxaliplatin while patients without detectable ctDNA and patients in the control group will standard follow-up according to guideline. The primary endpoint is the proportion of patients receiving ACT when ctDNA is detectable after resection. The main secondary outcome is 2-year recurrence rate (RR), but also includes 5-year RR, disease free survival, overall survival, time to recurrence, quality of life and cost-effectiveness. Data will be analyzed by intention to treat.
Discussion: The MEDOCC-CrEATE trial will provide insight into the willingness of stage II CC patients to be treated with ACT guided by ctDNA biomarker testing and whether ACT will prevent recurrences in a high-risk population. Use of the TwiCs design provides the opportunity to randomize patients before ctDNA measurement, avoiding ethical dilemmas of ctDNA status disclosure in the control group.
Trial registration: Netherlands Trial Register: NL6281/NTR6455 . Registered 18 May 2017, https://www.trialregister.nl/trial/6281.
Keywords: Adjuvant chemotherapy; Circulating tumor DNA; Colon cancer; TwiCs; ctDNA.
Conflict of interest statement
V.E.V. is a founder of Delfi Diagnostics and Personal Genome Diagnostics, serves on the Board of Directors and as a consultant for both organizations, and owns Delfi Diagnostics and Personal Genome Diagnostics stock, which are subject to certain restrictions under university policy. Additionally, Johns Hopkins University owns equity in Delfi Diagnostics and Personal Genome Diagnostics. V.E.V. is an advisor to Bristol-Myers Squibb, Genentech, Merck, and Takeda Pharmaceuticals. Within the last five years, V.E.V. has been an advisor to Daiichi Sankyo, Janssen Diagnostics, and Ignyta. These arrangements have been reviewed and approved by the Johns Hopkins University in accordance with its conflict of interest policies. J.P. is a founder of Delfi Diagnostics and owns Delfi Diagnostics stock.
Figures
References
-
- Bockelman C, Engelmann BE, Kaprio T, Hansen TF, Glimelius B. Risk of recurrence in patients with colon cancer stage II and III: a systematic review and meta-analysis of recent literature. Acta Oncol. 2015;54(1):5–16. - PubMed
-
- Quasar Collaborative Group. Gray R, Barnwell J, McConkey C, Hills RK, Williams NS, et al. Adjuvant chemotherapy versus observation in patients with colorectal cancer: a randomised study. Lancet. 2007;370(9604):2020–2029. - PubMed
-
- Andre T, de Gramont A, Vernerey D, Chibaudel B, Bonnetain F, Tijeras-Raballand A, et al. Adjuvant fluorouracil, Leucovorin, and Oxaliplatin in stage II to III Colon Cancer: updated 10-year survival and outcomes according to BRAF mutation and mismatch repair status of the MOSAIC study. J Clin Oncol. 2015;33(35):4176–4187. - PubMed
-
- Labianca R, Nordlinger B, Beretta GD, Mosconi S, Mandala M, Cervantes A, et al. Early colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(Suppl 6):vi64–vi72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
