

Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome: a comprehensive update
- PMID: 32819397
- PMCID: PMC7439721
- DOI: 10.1186/s13023-020-01491-9
Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome: a comprehensive update
Abstract
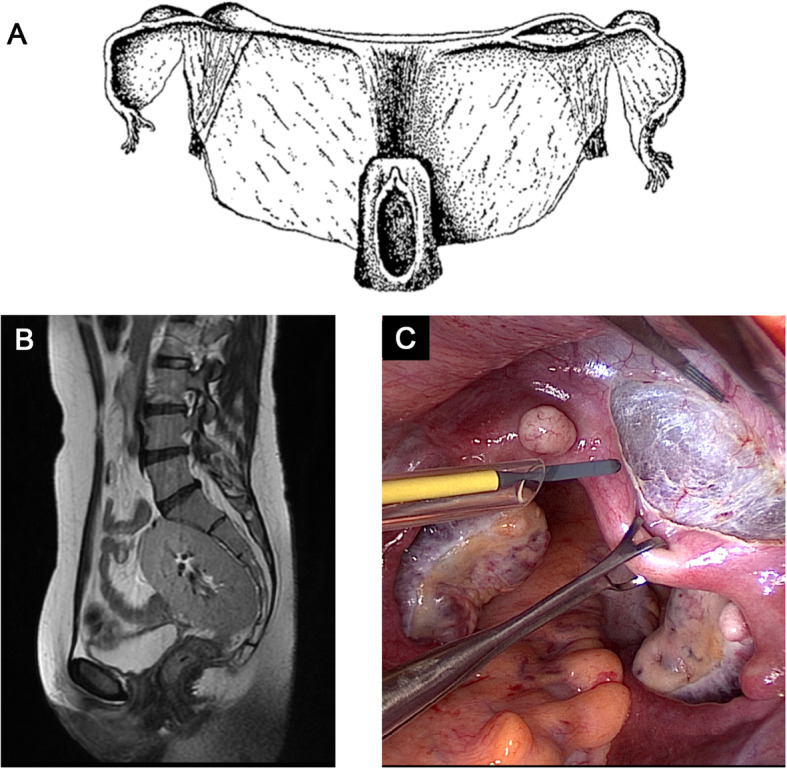
Background: Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome, also referred to as Müllerian aplasia, is a congenital disorder characterized by aplasia of the uterus and upper part of the vagina in females with normal secondary sex characteristics and a normal female karyotype (46,XX).
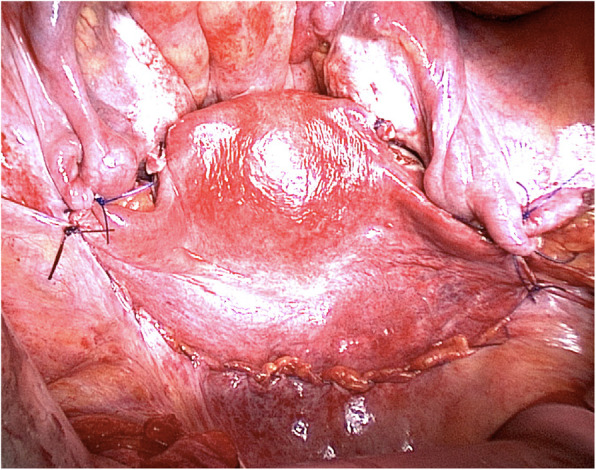
Main body: The diagnosis is often made during adolescence following investigations for primary amenorrhea and has an estimated prevalence of 1 in 5000 live female births. MRKH syndrome is classified as type I (isolated uterovaginal aplasia) or type II (associated with extragenital manifestations). Extragenital anomalies typically include renal, skeletal, ear, or cardiac malformations. The etiology of MRKH syndrome still remains elusive, however increasing reports of familial clustering point towards genetic causes and the use of various genomic techniques has allowed the identification of promising recurrent genetic abnormalities in some patients. The psychosexual impact of having MRKH syndrome should not be underestimated and the clinical care foremost involves thorough counselling and support in careful dialogue with the patient. Vaginal agenesis therapy is available for mature patients following therapeutical counselling and education with non-invasive vaginal dilations recommended as first-line therapy or by surgery. MRKH syndrome involves absolute uterine factor infertility and until recently, the only option for the patients to achieve biological motherhood was through gestational surrogacy, which is prohibited in most countries. However, the successful clinical trial of uterus transplantation (UTx) by a Swedish team followed by the first live-birth in September, 2014 in Gothenburg, proofed the first available fertility treatment in MRKH syndrome and UTx is now being performed in other countries around the world allowing women with MRKH syndrome to carry their own child and achieve biological motherhood.
Conclusion: Several advances in research across multiple disciplines have been made in the recent years and this kaleidoscopic review provides a current status of various key aspects in MRKH syndrome and provides perspectives for future research and improved clinical care.
Keywords: 46,XX DSD; Disorders of sex development; Female genitalia; Female infertility; Genetics; MRKH syndrome; MRKHS; Müllerian aplasia; Uterus transplantation; Vaginal agenesis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Timmreck LS, Reindollar RH. Contemporary issues in primary amenorrhea. Obstet Gynecol Clin N Am. 2003;30:287–302. - PubMed
-
- Aittomaki K, Eroila H, Kajanoja P. A population-based study of the incidence of Mullerian aplasia in Finland. Fertil Steril. 2001;76:624–625. - PubMed
-
- Herlin M, Bjørn A-MB, Rasmussen M, Trolle B, Petersen MB. Prevalence and patient characteristics of Mayer-Rokitansky-Küster-Hauser syndrome: a nationwide registry-based study. Hum Reprod. 2016;31:2384–2390. - PubMed
-
- Engstad JE. Artificial vagina. J Lancet. 1917;37:329–331.
-
- Owens N. Simplified method for formation of an artificial vagina by split skin graft. Report of a case. Surgery. 1942;12:139–150.
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
