

Angiotensin Converting Enzyme Inhibitor and Angiotensin II Receptor Blocker Use Among Outpatients Diagnosed With COVID-19
- PMID: 32819683
- PMCID: PMC7354276
- DOI: 10.1016/j.amjcard.2020.07.007
Angiotensin Converting Enzyme Inhibitor and Angiotensin II Receptor Blocker Use Among Outpatients Diagnosed With COVID-19
Abstract
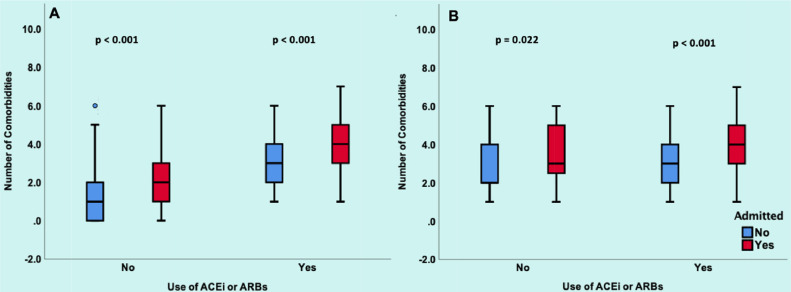
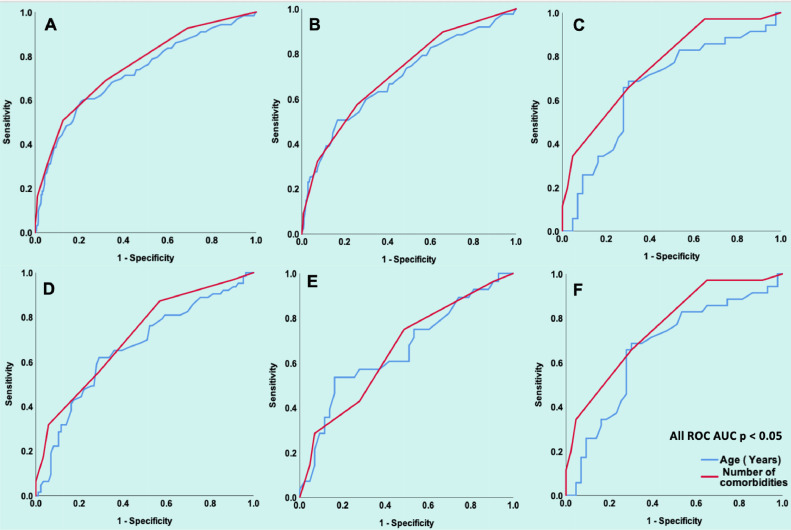
Coronavirus disease 2019 (COVID-19) is a viral pandemic precipitated by the severe acute respiratory syndrome coronavirus 2. Since previous reports suggested that viral entry into cells may involve angiotensin converting enzyme 2, there has been growing concern that angiotensin converting enzyme inhibitor (ACEI) and angiotensin II receptor blocker (ARB) use may exacerbate the disease severity. In this retrospective, single-center US study of adult patients diagnosed with COVID-19, we evaluated the association of ACEI/ARB use with hospital admission. Secondary outcomes included: ICU admission, mechanical ventilation, length of hospital stay, use of inotropes, and all-cause mortality. Propensity score matching was performed to account for potential confounders. Among 590 unmatched patients diagnosed with COVID-19, 78 patients were receiving ACEI/ARB (median age 63 years and 59.7% male) and 512 patients were non-users (median age 42 years and 47.1% male). In the propensity matched population, multivariate logistic regression analysis adjusting for age, gender and comorbidities demonstrated that ACEI/ARB use was not associated with hospital admission (OR 1.2, 95%CI 0.5 to 2.7, p = 0.652). CAD and CKD/end stage renal disease [ESRD] remained independently associated with admission to hospital. All-cause mortality, ICU stay, need for ventilation, and inotrope use was not significantly different between the 2 study groups. In conclusion, among patients who were diagnosed with COVID-19, ACEI/ARB use was not associated with increased risk of hospital admission.
Published by Elsevier Inc.
Conflict of interest statement
Conflict of Interests The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Anguiano L, Riera M, Pascual J, Valdivielso J, Barrios C, Betriu A, Mojal S, Fernandez E, Soler M. Circulating angiotensin-converting enzyme 2 activity in patients with chronic kidney disease without previous history of cardiovascular disease. Nephrol Dial Transplant. 2015;30:1176–1185. - PMC - PubMed
-
- Zhang P, Zhu L, Cai J, Qin JJ, Xie J, Liu YM, Zhao YC, Huang X, Lin L, Xia M, Chen MM, Cheng X, Zhang X, Guo D, Peng Y, Ji YX, Chen J, Shen ZG, Wang Y, Xu Q, Tan R, Wang H, Lin J, Luo P, Fu S, Cai H, Ye P, Xiao B, Mao W, Liu L, Yan Y, Liu M, Chen M, Zhang XJ, Wang X, Touyz RM, Xia J, Zhang BH, Huang X, Yuan Y, Rohit L, Liu PP, Li H. Association of inpatient use of angiotensin converting enzyme inhibitors and angiotensin II receptor blockers with mortality among patients with hypertension hospitalized With COVID-19. Circ Res. 2020 doi: 10.1161/CIRCRESAHA.120.317134. [E-pub ahead of print] - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
