

Thin-Section MR Imaging for Carotid Cavernous Fistula
- PMID: 32819900
- PMCID: PMC7583100
- DOI: 10.3174/ajnr.A6757
Thin-Section MR Imaging for Carotid Cavernous Fistula
Abstract
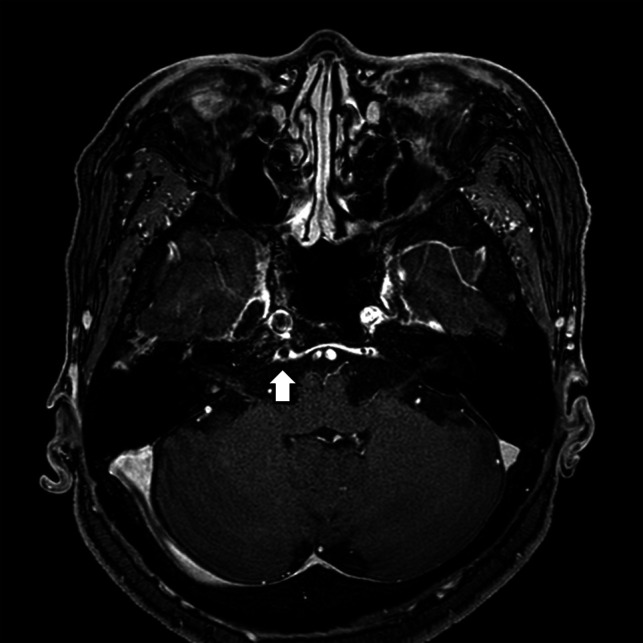
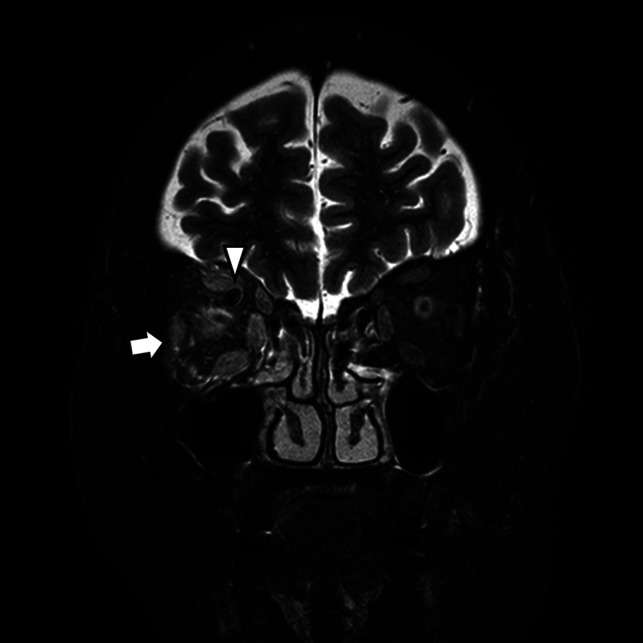
Background and purpose: Carotid-cavernous fistulas are abnormal vascular shunts that can cause various neurologic or orbital symptoms. The purpose of this retrospective study was to evaluate the diagnostic performance of thin-section MR imaging for carotid cavernous fistula in patients with clinically suspected carotid cavernous fistula, and to identify possible imaging predictors of carotid cavernous fistula.
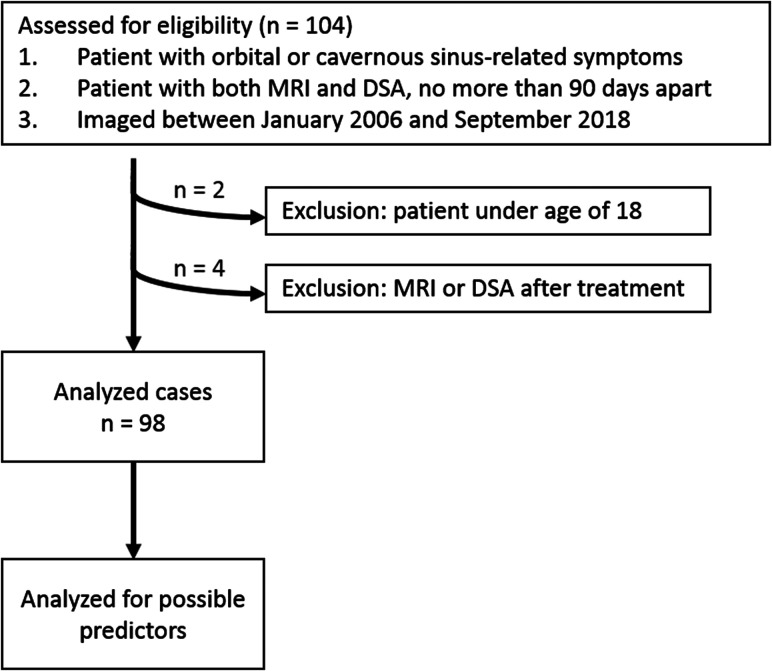
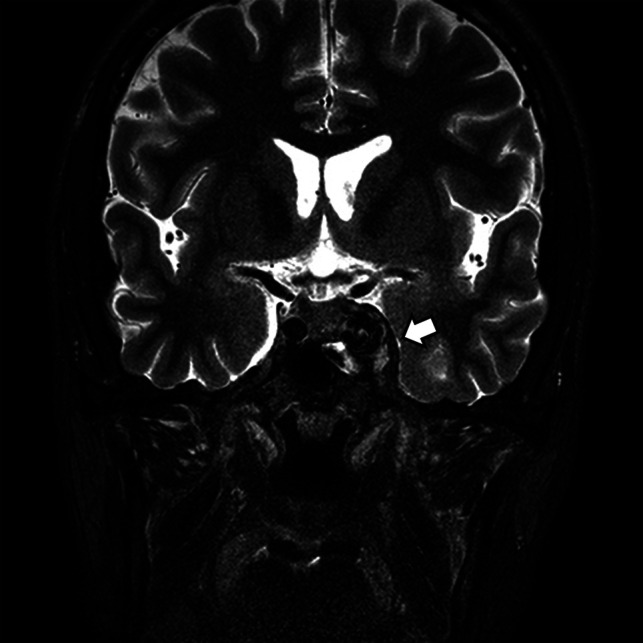
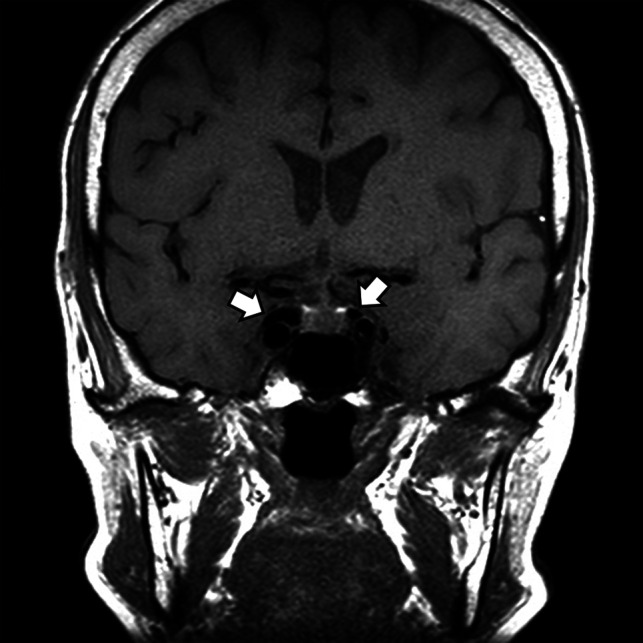
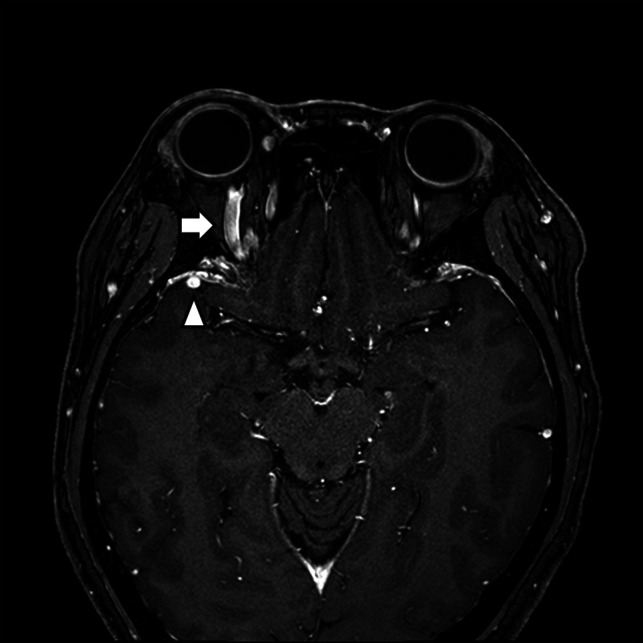
Materials and methods: A total of 98 patients who were clinically suspected of having carotid cavernous fistula (according to their symptoms and physical examinations) between January 2006 and September 2018 were included in this study. The patients underwent pretreatment thin-section MR imaging and DSA. Thin-section MR imaging consisted of 2D coronal T1- and T2WI with 3-mm thickness and 3D contrast-enhanced T1WI with 0.6 mm thickness. The diagnostic performance of thin-section MR imaging for carotid cavernous fistula was evaluated with the reference standard of DSA. Univariate logistic regression analysis was performed to determine possible imaging predictors of carotid cavernous fistula.
Results: Among the 98 patients, DSA confirmed 38 as having carotid cavernous fistula. The overall accuracy, sensitivity, and specificity of thin-section MR imaging were 88.8%, 97.4%, and 83.3%, respectively. Possible imaging predictors on thin-section MR imaging included abnormal contour of the cavernous sinus (OR: 21.7), internal signal void of the cavernous sinus (OR: 15.3), prominent venous drainage flow (OR: 54.0), and orbital/periorbital soft tissue swelling (OR: 40.4).
Conclusions: Thin-section MR imaging provides high diagnostic performance and possible imaging predictors of carotid cavernous fistula in patients with clinically suspected carotid cavernous fistula. Thin-section MR imaging protocols could help decide appropriate management plans for patients with clinically suspected carotid cavernous fistula.
© 2020 by American Journal of Neuroradiology.
Figures
Similar articles
-
Evaluating the diagnostic performance of non-contrast magnetic resonance angiography sequences in the pre-procedural comprehensive analysis of direct carotid cavernous fistula.Neuroradiology. 2024 Jul;66(7):1203-1212. doi: 10.1007/s00234-024-03342-x. Epub 2024 Apr 6. Neuroradiology. 2024. PMID: 38581636
-
CT angiography and MR angiography in the evaluation of carotid cavernous sinus fistula prior to embolization: a comparison of techniques.AJNR Am J Neuroradiol. 2005 Oct;26(9):2349-56. AJNR Am J Neuroradiol. 2005. PMID: 16219844 Free PMC article.
-
Parametric color coding of digital subtraction angiography in the evaluation of carotid cavernous fistulas.Clin Neuroradiol. 2013 Jun;23(2):113-20. doi: 10.1007/s00062-012-0184-8. Epub 2012 Dec 14. Clin Neuroradiol. 2013. PMID: 23241650
-
Carotid-cavernous and orbital arteriovenous fistulas: ocular features, diagnostic and hemodynamic considerations in relation to visual impairment and morbidity.Orbit. 2003 Jun;22(2):121-42. doi: 10.1076/orbi.22.2.121.14315. Orbit. 2003. PMID: 12789591 Review.
-
Spontaneous resolution of direct carotid-cavernous fistulas: case series and literature review.Interv Neuroradiol. 2019 Feb;25(1):71-89. doi: 10.1177/1591019918800220. Epub 2018 Sep 23. Interv Neuroradiol. 2019. PMID: 30244626 Free PMC article. Review.
Cited by
-
Clinical Profiles and Treatment Outcomes of 51 Cases of Carotid Cavernous Fistula: A Retrospective Observational Study.Korean J Ophthalmol. 2025 Apr;39(2):181-188. doi: 10.3341/kjo.2024.0113. Epub 2025 Mar 10. Korean J Ophthalmol. 2025. PMID: 40059350 Free PMC article.
-
Evaluating the diagnostic performance of non-contrast magnetic resonance angiography sequences in the pre-procedural comprehensive analysis of direct carotid cavernous fistula.Neuroradiology. 2024 Jul;66(7):1203-1212. doi: 10.1007/s00234-024-03342-x. Epub 2024 Apr 6. Neuroradiology. 2024. PMID: 38581636
-
Pediatric orbital lesions: non-neoplastic extraocular soft-tissue lesions.Pediatr Radiol. 2024 May;54(6):910-921. doi: 10.1007/s00247-024-05892-x. Epub 2024 Feb 28. Pediatr Radiol. 2024. PMID: 38413469
-
Comparison of Single- and Multi-Echo Susceptibility-Weighted Imaging in Detecting Cerebral Arteriovenous Shunts: A Preliminary Study.J Korean Soc Radiol. 2023 Jan;84(1):226-239. doi: 10.3348/jksr.2022.0080. Epub 2023 Jan 30. J Korean Soc Radiol. 2023. PMID: 36818708 Free PMC article.
-
Extraocular muscle enlargement.Graefes Arch Clin Exp Ophthalmol. 2022 Nov;260(11):3419-3435. doi: 10.1007/s00417-022-05727-1. Epub 2022 Jun 17. Graefes Arch Clin Exp Ophthalmol. 2022. PMID: 35713708 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical