

Effects of empagliflozin and target-organ damage in a novel rodent model of heart failure induced by combined hypertension and diabetes
- PMID: 32820187
- PMCID: PMC7441148
- DOI: 10.1038/s41598-020-70708-5
Effects of empagliflozin and target-organ damage in a novel rodent model of heart failure induced by combined hypertension and diabetes
Abstract
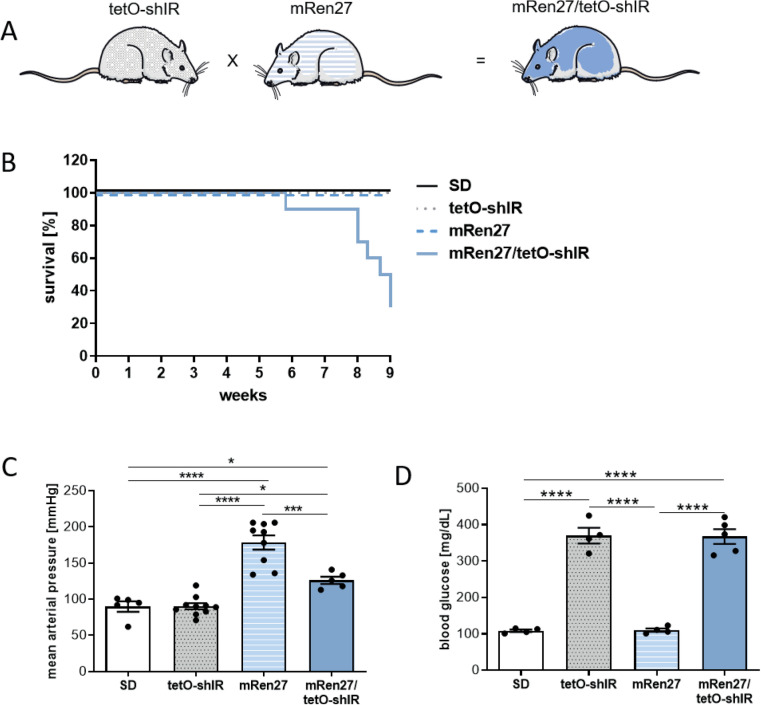
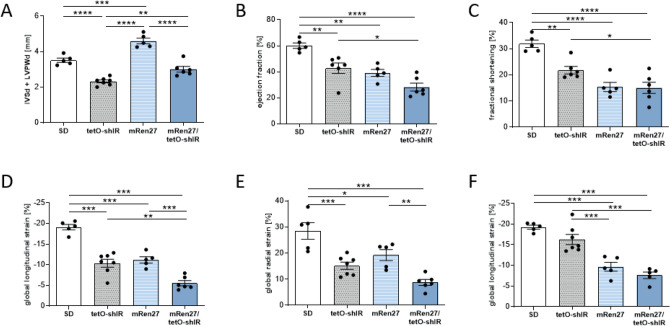
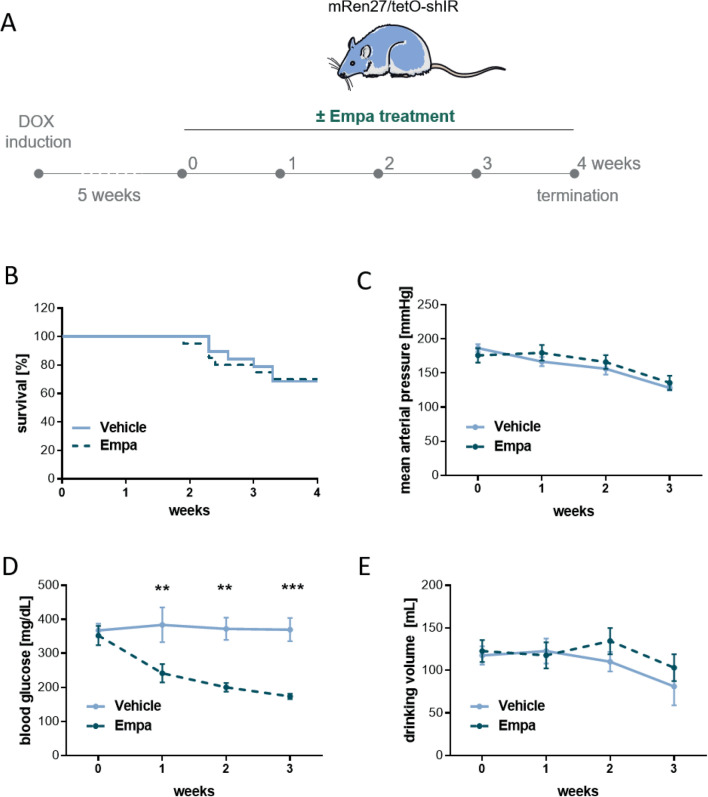
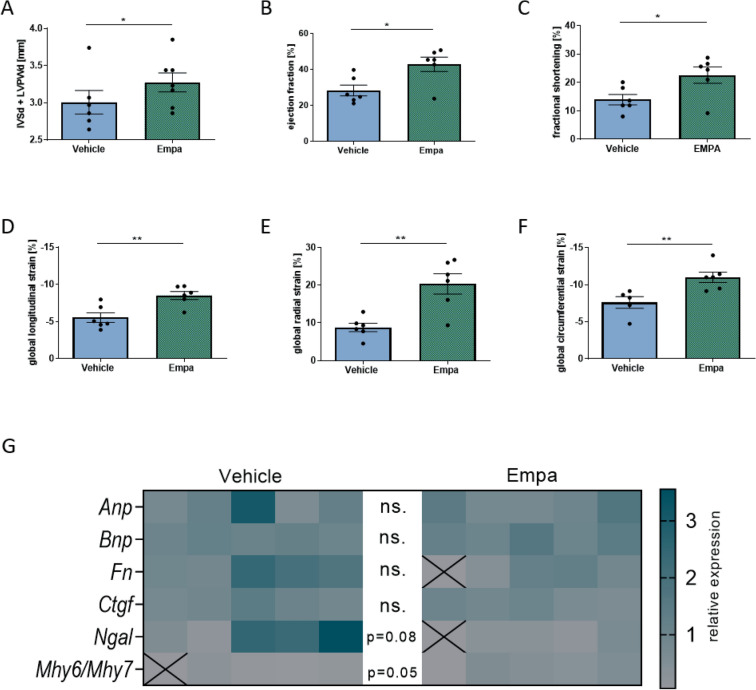
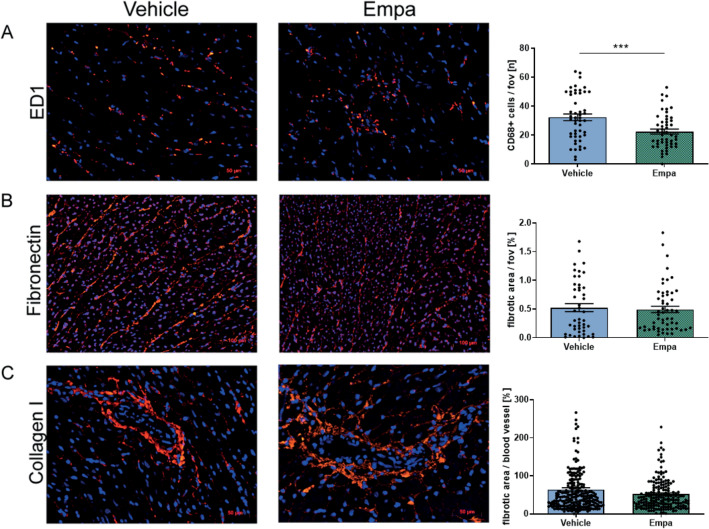
Type 2 diabetes mellitus and hypertension are two major risk factors leading to heart failure and cardiovascular damage. Lowering blood sugar by the sodium-glucose co-transporter 2 inhibitor empagliflozin provides cardiac protection. We established a new rat model that develops both inducible diabetes and genetic hypertension and investigated the effect of empagliflozin treatment to test the hypothesis if empagliflozin will be protective in a heart failure model which is not based on a primary vascular event. The transgenic Tet29 rat model for inducible diabetes was crossed with the mRen27 hypertensive rat to create a novel model for heart failure with two stressors. The diabetic, hypertensive heart failure rat (mRen27/tetO-shIR) were treated with empagliflozin (10 mg/kg/d) or vehicle for 4 weeks. Cardiovascular alterations were monitored by advanced speckle tracking echocardiography, gene expression analysis and immunohistological staining. The novel model with increased blood pressure und higher blood sugar levels had a reduced survival compared to controls. The rats develop heart failure with reduced ejection fraction. Empagliflozin lowered blood sugar levels compared to vehicle treated animals (182.3 ± 10.4 mg/dl vs. 359.4 ± 35.8 mg/dl) but not blood pressure (135.7 ± 10.3 mmHg vs. 128.2 ± 3.8 mmHg). The cardiac function was improved in all three global strains (global longitudinal strain - 8.5 ± 0.5% vs. - 5.5 ± 0.6%, global radial strain 20.4 ± 2.7% vs. 8.8 ± 1.1%, global circumferential strain - 11.0 ± 0.7% vs. - 7.6 ± 0.8%) and by increased ejection fraction (42.8 ± 4.0% vs. 28.2 ± 3.0%). In addition, infiltration of macrophages was decreased by treatment (22.4 ± 1.7 vs. 32.3 ± 2.3 per field of view), despite mortality was not improved. Empagliflozin showed beneficial effects on cardiovascular dysfunction. In this novel rat model of combined hypertension and diabetes, the improvement in systolic and diastolic function was not secondary to a reduction in left ventricular mass or through modulation of the afterload, since blood pressure was not changed. The mRen27/tetO-shIR strain should provide utility in separating blood sugar from blood pressure-related treatment effects.
Conflict of interest statement
RD has have served as advisor for Boehringer Ingelheim and has lectured on empaglifozin. UK took part on an Advisory Board from Boehringer Ingelheim. The rest of the authors have no competing interests.
Figures
Similar articles
-
The sodium-glucose co-transporter 2 inhibitor empagliflozin attenuates cardiac fibrosis and improves ventricular hemodynamics in hypertensive heart failure rats.Cardiovasc Diabetol. 2019 Apr 1;18(1):45. doi: 10.1186/s12933-019-0849-6. Cardiovasc Diabetol. 2019. PMID: 30935417 Free PMC article.
-
Load-independent effects of empagliflozin contribute to improved cardiac function in experimental heart failure with reduced ejection fraction.Cardiovasc Diabetol. 2020 Feb 8;19(1):13. doi: 10.1186/s12933-020-0994-y. Cardiovasc Diabetol. 2020. PMID: 32035482 Free PMC article.
-
Evaluation of the effect of sodium-glucose co-transporter 2 inhibition with empagliflozin on morbidity and mortality of patients with chronic heart failure and a reduced ejection fraction: rationale for and design of the EMPEROR-Reduced trial.Eur J Heart Fail. 2019 Oct;21(10):1270-1278. doi: 10.1002/ejhf.1536. Epub 2019 Jul 16. Eur J Heart Fail. 2019. PMID: 31584231
-
An evaluation of empagliflozin and it's applicability to hypertension as a therapeutic option.Expert Opin Pharmacother. 2020 Jul;21(10):1157-1166. doi: 10.1080/14656566.2020.1751815. Epub 2020 Apr 17. Expert Opin Pharmacother. 2020. PMID: 32301361 Review.
-
Empagliflozin in the treatment of heart failure.Future Cardiol. 2024 Apr 25;20(5-6):251-261. doi: 10.1080/14796678.2024.2360818. Epub 2024 Jun 12. Future Cardiol. 2024. PMID: 38865086 Free PMC article. Review.
Cited by
-
Suppression of Cardiogenic Edema with Sodium-Glucose Cotransporter-2 Inhibitors in Heart Failure with Reduced Ejection Fraction: Mechanisms and Insights from Pre-Clinical Studies.Biomedicines. 2022 Aug 19;10(8):2016. doi: 10.3390/biomedicines10082016. Biomedicines. 2022. PMID: 36009562 Free PMC article. Review.
-
Traditional Chinese Medicine Ginseng Dingzhi Decoction Ameliorates Myocardial Fibrosis and High Glucose-Induced Cardiomyocyte Injury by Regulating Intestinal Flora and Mitochondrial Dysfunction.Oxid Med Cell Longev. 2022 Mar 31;2022:9205908. doi: 10.1155/2022/9205908. eCollection 2022. Oxid Med Cell Longev. 2022. PMID: 35401934 Free PMC article.
-
Role and molecular mechanisms of SGLT2 inhibitors in pathological cardiac remodeling (Review).Mol Med Rep. 2024 May;29(5):73. doi: 10.3892/mmr.2024.13197. Epub 2024 Mar 15. Mol Med Rep. 2024. PMID: 38488029 Free PMC article. Review.
-
Role of Sodium-Glucose Co-Transporter 2 Inhibitors in the Regulation of Inflammatory Processes in Animal Models.Int J Mol Sci. 2022 May 18;23(10):5634. doi: 10.3390/ijms23105634. Int J Mol Sci. 2022. PMID: 35628443 Free PMC article. Review.
-
Effects of SGLT2 inhibitor administration on blood glucose level and body weight in type 1 diabetes rat model.Narra J. 2023 Aug;3(2):e194. doi: 10.52225/narra.v3i2.194. Epub 2023 Aug 31. Narra J. 2023. PMID: 38450274 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
