

Ultraconservative, Fertility Sparing Treatment of Bilateral Borderline Ovarian Tumors: A Case Report of a 26-Year-Old, 0-Gravida with an Endometrioid Borderline Ovarian Tumor of the Right Ovary and a Sero-Mucinous Borderline Ovarian Tumor of the Left Ovary and a Review of the Literature
- PMID: 32821173
- PMCID: PMC7418455
- DOI: 10.2147/IJWH.S258478
Ultraconservative, Fertility Sparing Treatment of Bilateral Borderline Ovarian Tumors: A Case Report of a 26-Year-Old, 0-Gravida with an Endometrioid Borderline Ovarian Tumor of the Right Ovary and a Sero-Mucinous Borderline Ovarian Tumor of the Left Ovary and a Review of the Literature
Abstract
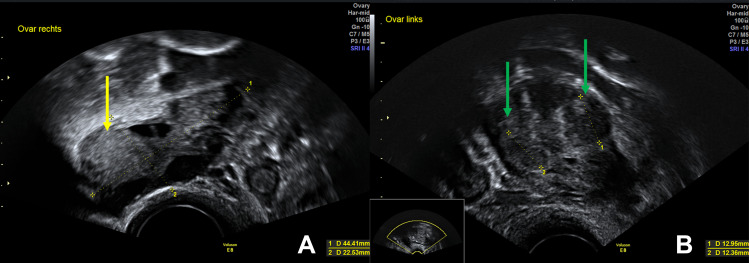
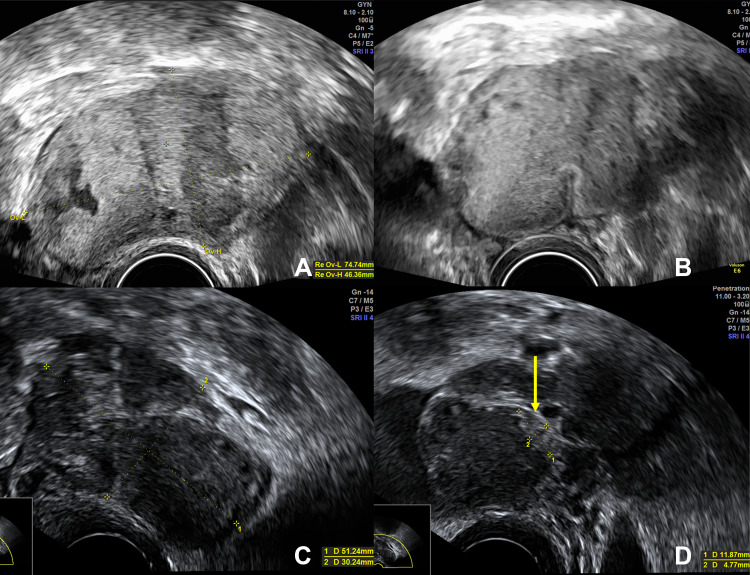
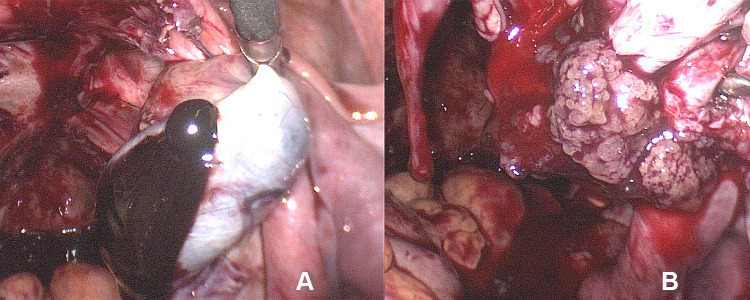
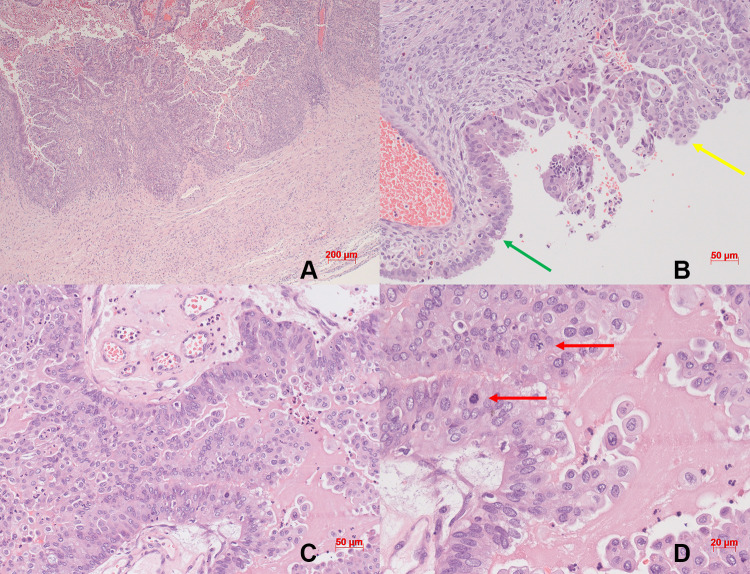
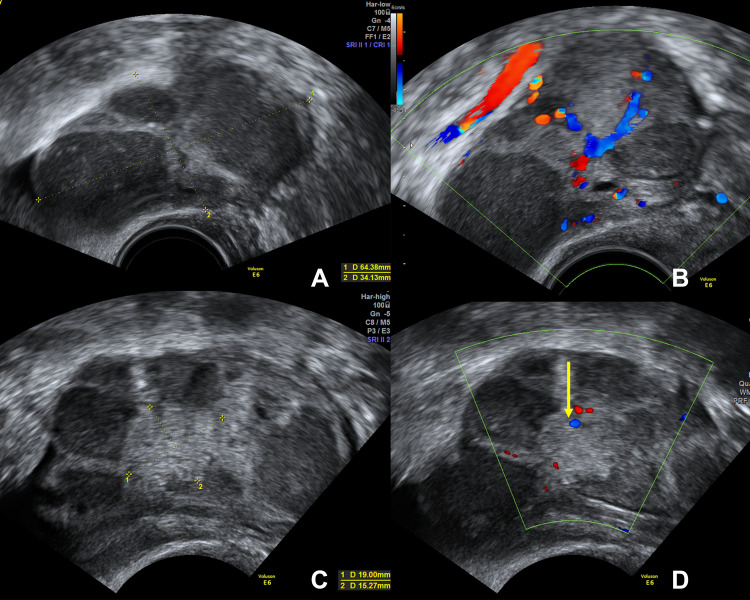
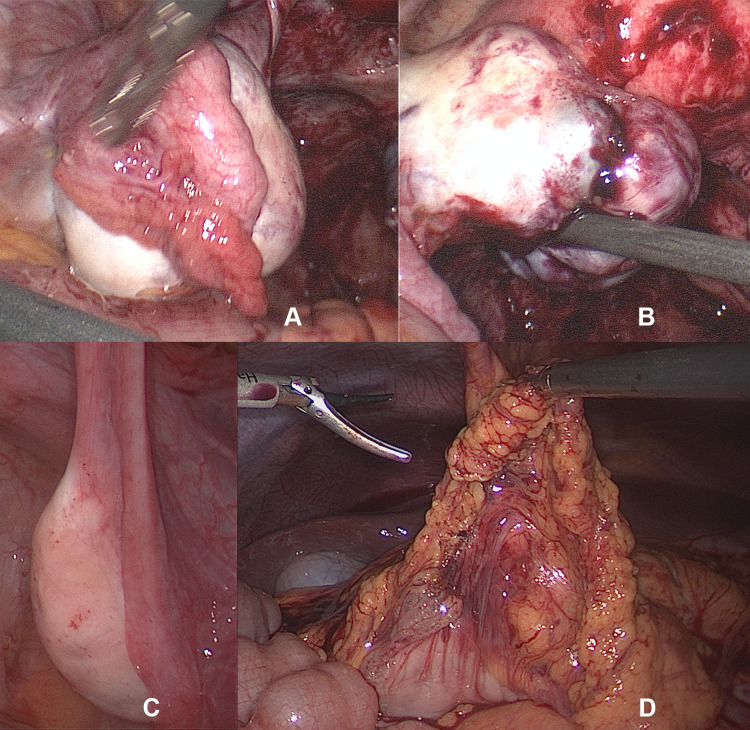
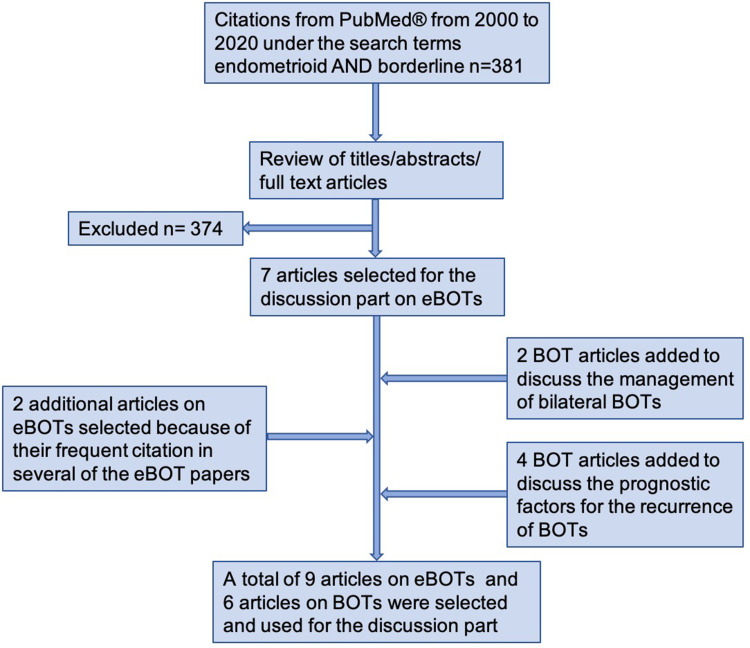
Endometrioid borderline ovarian tumors are rare, entailing a lack of data on their natural history as well as the safety of conservative and ultraconservative surgical management, especially in cases with bilateral borderline ovarian tumors including one of endometrioid differentiation. Therefore, we present such a case and provide a review of the literature on endometrioid borderline ovarian tumors. We report the case of a 26-year-old, 0-gravida with an endometrioid borderline ovarian tumor of the right and a sero-mucinous borderline ovarian tumor of the left ovary treated by fertility sparing, ultraconservative surgery with bilateral cystectomy, completed by staging procedures including omentectomy and peritoneal sampling, as well as endometrial sampling by means of curettage. Reviewing the literature and taking into account the course of our case, we propose the feasibility of an ultraconservative management, including endometrial sampling, in young patients with bilateral borderline ovarian tumors including one of endometrioid differentiation who desire to preserve fertility, followed by a closely monitored follow-up.
Keywords: bilateral borderline ovarian tumor; bilateral cystectomy; endometrioid borderline ovarian tumor; fertility sparing surgery; ultraconservative treatment.
© 2020 Verta and Kipp.
Conflict of interest statement
Both authors report no conflicts of interest in this work.
Figures
Similar articles
-
[Borderline Ovarian Tumours: CNGOF Guidelines for Clinical Practice - Therapeutic Management of Early Stages].Gynecol Obstet Fertil Senol. 2020 Mar;48(3):287-303. doi: 10.1016/j.gofs.2020.01.016. Epub 2020 Jan 28. Gynecol Obstet Fertil Senol. 2020. PMID: 32004786 French.
-
The impact of clinicopathologic and surgical factors on relapse and pregnancy in young patients (≤40 years old) with borderline ovarian tumors.BMC Cancer. 2018 Nov 21;18(1):1147. doi: 10.1186/s12885-018-4932-2. BMC Cancer. 2018. PMID: 30463533 Free PMC article.
-
A patient with a mucinous borderline ovarian tumor after fertility-sparing surgery in whom puncture fluid cytology on oocyte retrieval led to a diagnosis of recurrence.J Obstet Gynaecol Res. 2022 Oct;48(10):2635-2639. doi: 10.1111/jog.15365. Epub 2022 Jul 24. J Obstet Gynaecol Res. 2022. PMID: 35871537
-
Conservative management of epithelial ovarian cancer.Eur J Gynaecol Oncol. 2005;26(5):473-8. Eur J Gynaecol Oncol. 2005. PMID: 16285560 Review.
-
Management of borderline ovarian neoplasms.J Clin Oncol. 2007 Jul 10;25(20):2928-37. doi: 10.1200/JCO.2007.10.8076. J Clin Oncol. 2007. PMID: 17617524 Review.
Cited by
-
The Role of Myeloid-Derived Suppressor Cells (MDSCs) in the Development and/or Progression of Endometriosis-State of the Art.Cells. 2021 Mar 18;10(3):677. doi: 10.3390/cells10030677. Cells. 2021. PMID: 33803806 Free PMC article. Review.
-
Clinical Characteristics, Surgical Management, and Outcomes of Borderline Ovarian Tumours: A Retrospective Observational Study from North East London.J Clin Med. 2025 Mar 30;14(7):2383. doi: 10.3390/jcm14072383. J Clin Med. 2025. PMID: 40217833 Free PMC article.
-
Management of Borderline ovarian tumors (BOT): results of a retrospective, single center study in Switzerland.J Ovarian Res. 2023 Jan 23;16(1):20. doi: 10.1186/s13048-023-01107-3. J Ovarian Res. 2023. PMID: 36691070 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
