

Association of Neighborhood Disadvantage With Cardiovascular Risk Factors and Events Among Refugees in Denmark
- PMID: 32821923
- PMCID: PMC7442927
- DOI: 10.1001/jamanetworkopen.2020.14196
Association of Neighborhood Disadvantage With Cardiovascular Risk Factors and Events Among Refugees in Denmark
Abstract
Importance: Refugees are among the most disadvantaged individuals in society, and they often have elevated risks of cardiovascular risk factors and events. Evidence is limited regarding factors that may worsen cardiovascular health among this vulnerable group.
Objective: To test the hypothesis that refugee placement in socioeconomically disadvantaged neighborhoods is associated with increased cardiovascular risk.
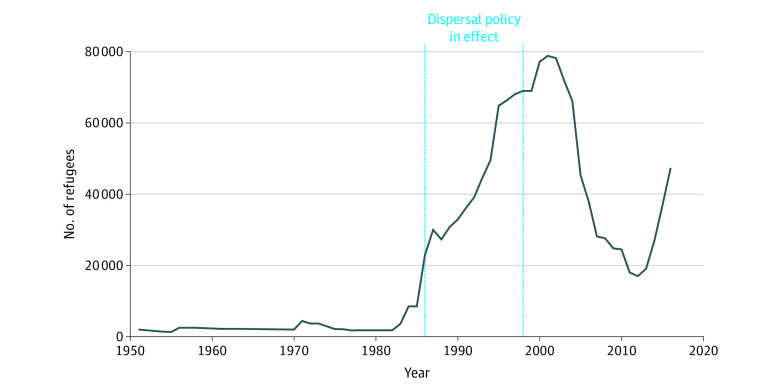
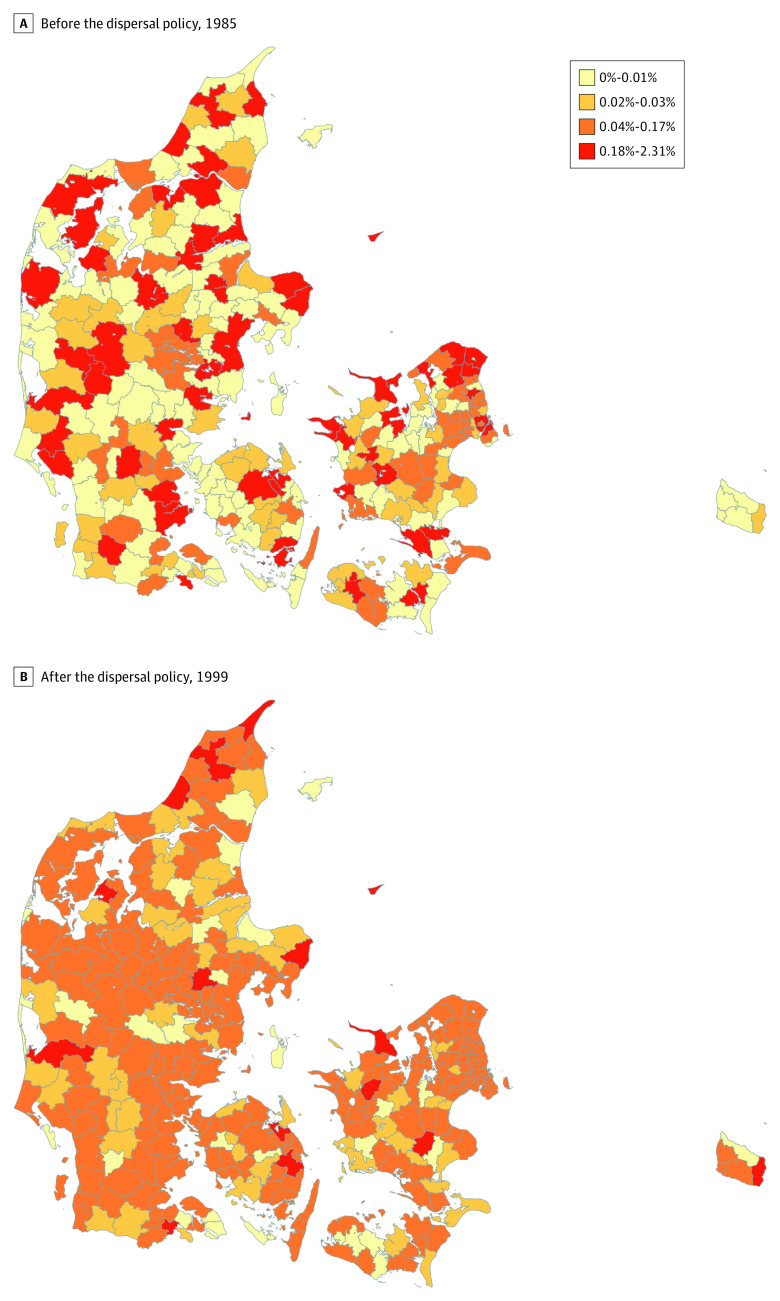
Design, setting, and participants: The study population of this quasi-experimental, registry-based cohort study included 49 305 adults 18 years and older who came to Denmark as refugees from other countries during the years of Denmark's refugee dispersal policy from 1986 to 1998. Refugees were dispersed to neighborhoods with varying degrees of socioeconomic disadvantage in an arbitrary manner conditional on observed characteristics. The association of neighborhood disadvantage on arrival with several cardiovascular outcomes in subsequent decades was evaluated using regression models that adjusted for individual, family, and municipal characteristics. Health outcomes were abstracted from the inpatient register, outpatient specialty clinic register, and prescription drug register through 2016. Data analysis was conducted from May 2018 to July 2019.
Exposures: A composite index of neighborhood disadvantage was constructed using 8 neighborhood-level socioeconomic characteristics derived from Danish population register data.
Main outcomes and measures: Primary study outcomes included hypertension, hyperlipidemia, type 2 diabetes, myocardial infarction, and stroke. Before data analysis commenced, it was hypothesized that higher levels of neighborhood disadvantage were associated with an increased risk of cardiovascular risk factors and events.
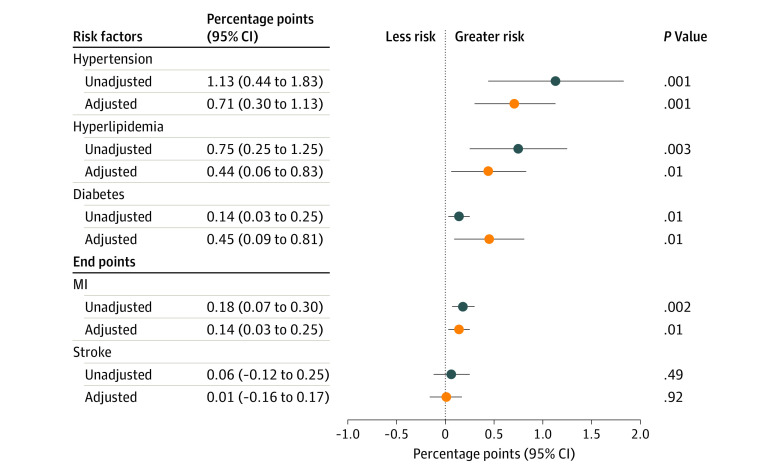
Results: A total of 49 305 participants were included (median [interquartile range] age, 30.5 [24.9-39.8] years; 43.3% women). Participant region of origin included 6318 from Africa (12.8%), 7253 from Asia (14.7%), 3446 from Eastern Europe (7.0%), 5416 from Iraq (11.0%), 6206 from Iran (12.6%), 5558 from Palestine (via Lebanon, Israel, Occupied Palestinian Territories; 11.3%), and 15 108 from Yugoslavia (30.6%). Adjusted models revealed an association between placement in disadvantaged neighborhoods and increased risk of hypertension (0.71 [95% CI, 0.30-1.13] percentage points per unit of disadvantage index; P < .01), hyperlipidemia (0.44 [95% CI, 0.06-0.83] percentage points; P = .01), diabetes (0.45 [95% CI, 0.09-0.81] percentage points; P = .01), and myocardial infarction (0.14 [95% CI, 0.03-0.25] percentage points; P = .01). No association was found for stroke. Individuals who arrived in Denmark before age 35 years had an increased risk of hyperlipidemia (1.16 [95% CI, 0.41-1.92] percentage points; P < .01), and there were no differences by sex.
Conclusions and relevance: In this quasi-experimental cohort study, neighborhood disadvantage was associated with increased cardiovascular risk in a relatively young population of refugees. Neighborhood characteristics may be an important consideration when refugees are placed by resettlement agencies and host countries. Future work should examine additional health outcomes as well as potential mediating pathways to target future interventions (eg, neighborhood ease of walking, employment opportunities).
Conflict of interest statement
Figures
Comment in
-
Neighborhood Environment Has a Profound Association With Refugees' Health.JAMA Netw Open. 2020 Aug 3;3(8):e2014355. doi: 10.1001/jamanetworkopen.2020.14355. JAMA Netw Open. 2020. PMID: 32821918 No abstract available.
References
-
- Markides KS, Rote S. Immigrant health paradox In: Scott RA, Kosslyn SM, eds. Emerging Trends in the Social and Behavioral Sciences. John Wiley & Sons; 2015. doi:10.1002/9781118900772.etrds0174 - DOI
-
- Connor P. Explaining the refugee gap: economic outcomes of refugees versus other immigrants. J Refug Stud. 2010;23(3):377-397. doi:10.1093/jrs/feq025 - DOI
