

What's New for Clinical Whole-body MRI (WB-MRI) in the 21st Century
- PMID: 32822545
- PMCID: PMC8519652
- DOI: 10.1259/bjr.20200562
What's New for Clinical Whole-body MRI (WB-MRI) in the 21st Century
Abstract
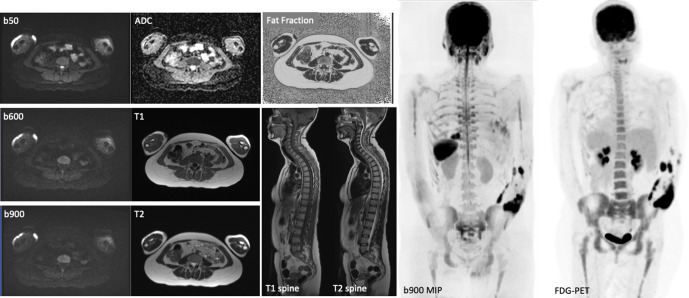
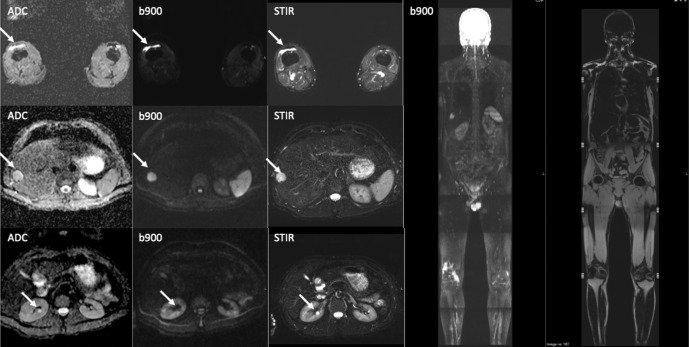
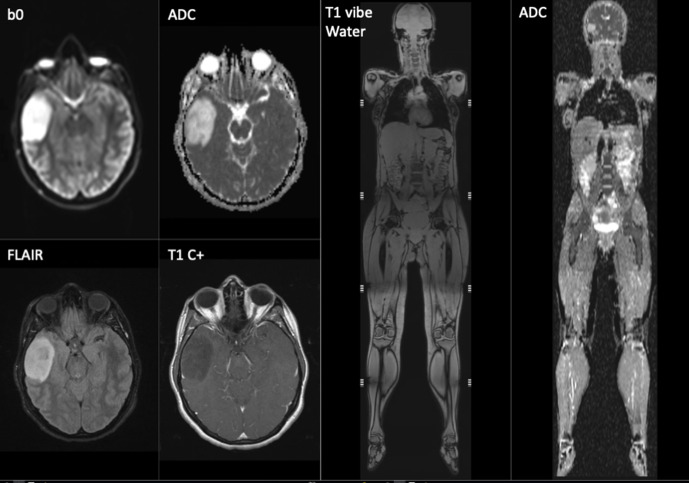
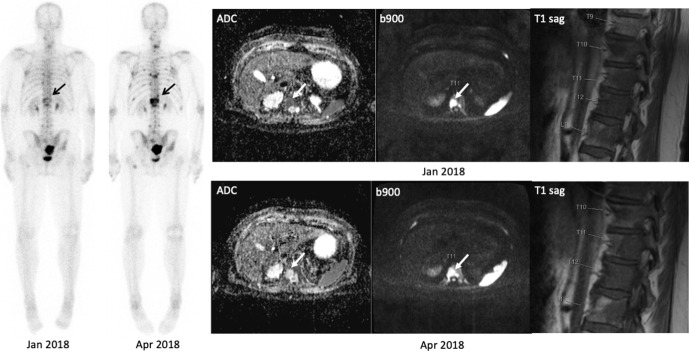
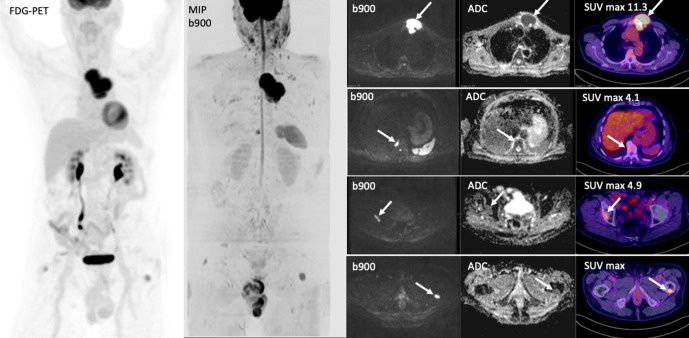
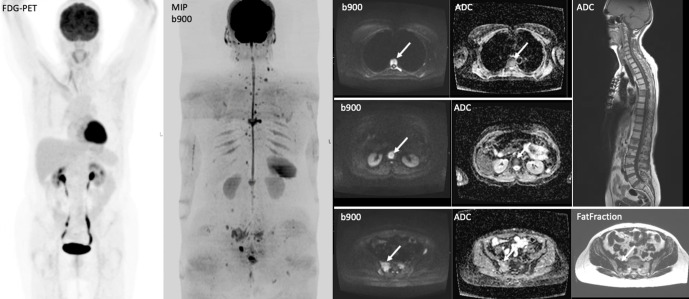
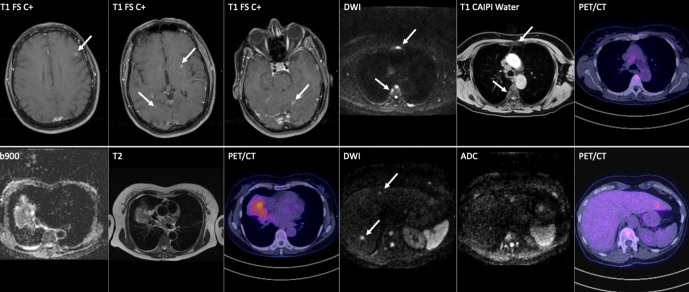
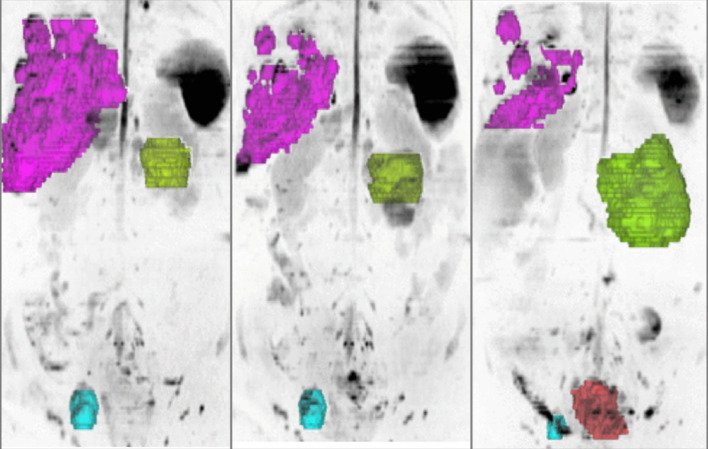
Whole-body MRI (WB-MRI) has evolved since its first introduction in the 1970s as an imaging technique to detect and survey disease across multiple sites and organ systems in the body. The development of diffusion-weighted MRI (DWI) has added a new dimension to the implementation of WB-MRI on modern scanners, offering excellent lesion-to-background contrast, while achieving acceptable spatial resolution to detect focal lesions 5 to 10 mm in size. MRI hardware and software advances have reduced acquisition times, with studies taking 40-50 min to complete.The rising awareness of medical radiation exposure coupled with the advantages of MRI has resulted in increased utilization of WB-MRI in oncology, paediatrics, rheumatological and musculoskeletal conditions and more recently in population screening. There is recognition that WB-MRI can be used to track disease evolution and monitor response heterogeneity in patients with cancer. There are also opportunities to combine WB-MRI with molecular imaging on PET-MRI systems to harness the strengths of hybrid imaging. The advent of artificial intelligence and machine learning will shorten image acquisition times and image analyses, making the technique more competitive against other imaging technologies.
Figures

References
-
- Taylor SA, Mallett S, Beare S, Bhatnagar G, Blunt D, Boavida P, et al. Diagnostic accuracy of whole-body MRI versus standard imaging pathways for metastatic disease in newly diagnosed colorectal cancer: the prospective streamline C trial. Lancet Gastroenterol Hepatol 2019; 4: 529–37. doi: 10.1016/S2468-1253(19)30056-1 - DOI - PMC - PubMed
-
- Taylor SA, Mallett S, Ball S, Beare S, Bhatnagar G, Bhowmik A, et al. Diagnostic accuracy of whole-body MRI versus standard imaging pathways for metastatic disease in newly diagnosed non-small-cell lung cancer: the prospective streamline L trial. Lancet Respir Med 2019; 7: 523–32. doi: 10.1016/S2213-2600(19)30090-6 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
