

Considering Cause and Effect of Immune Cell Aging on Cardiac Repair after Myocardial Infarction
- PMID: 32823583
- PMCID: PMC7465938
- DOI: 10.3390/cells9081894
Considering Cause and Effect of Immune Cell Aging on Cardiac Repair after Myocardial Infarction
Abstract
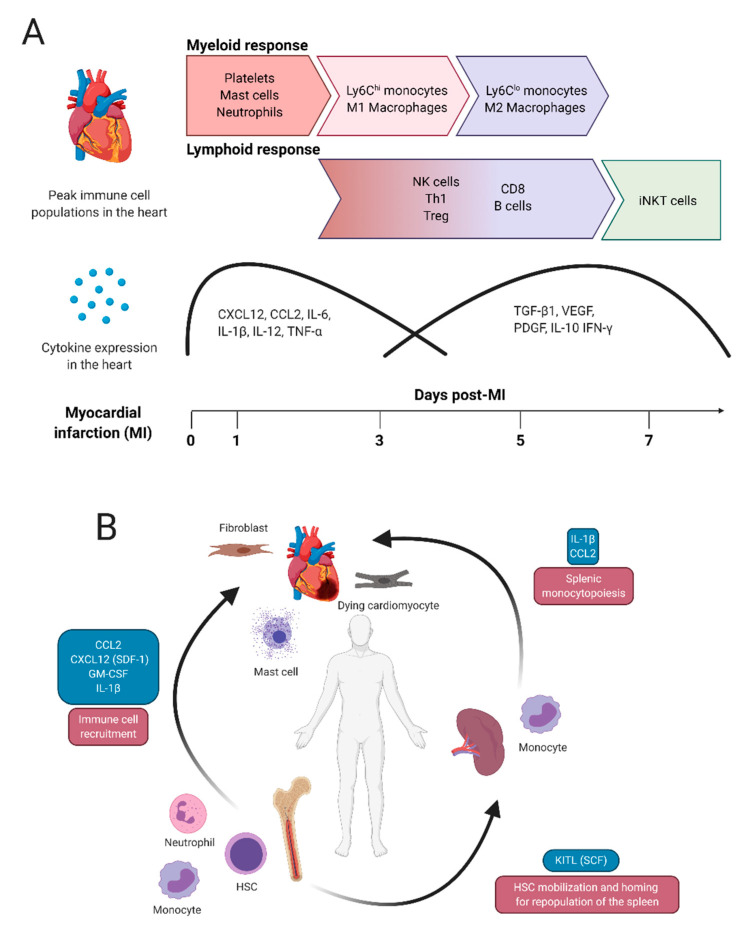
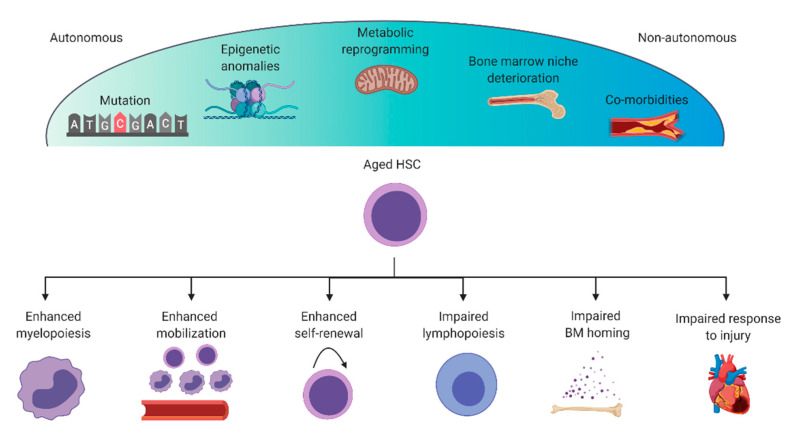
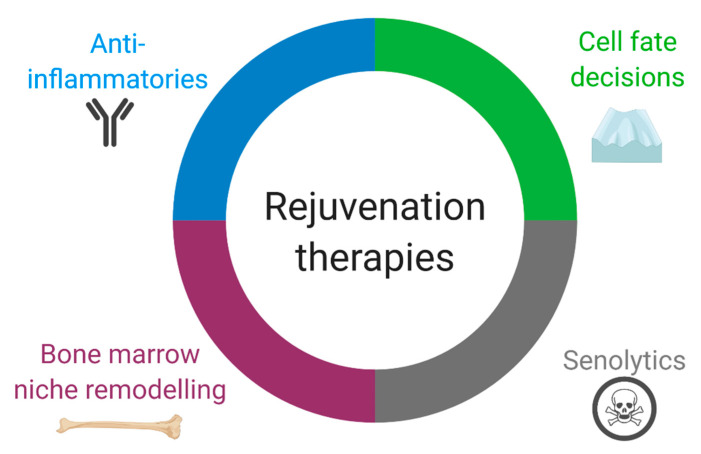
The importance of the immune system for cardiac repair following myocardial infarction is undeniable; however, the complex nature of immune cell behavior has limited the ability to develop effective therapeutics. This limitation highlights the need for a better understanding of the function of each immune cell population during the inflammatory and resolution phases of cardiac repair. The development of reliable therapies is further complicated by aging, which is associated with a decline in cell and organ function and the onset of cardiovascular and immunological diseases. Aging of the immune system has important consequences on heart function as both chronic cardiac inflammation and an impaired immune response to cardiac injury are observed in older individuals. Several studies have suggested that rejuvenating the aged immune system may be a valid therapeutic candidate to prevent or treat heart disease. Here, we review the basic patterns of immune cell behavior after myocardial infarction and discuss the autonomous and nonautonomous manners of hematopoietic stem cell and immune cell aging. Lastly, we identify prospective therapies that may rejuvenate the aged immune system to improve heart function such as anti-inflammatory and senolytic therapies, bone marrow transplant, niche remodeling and regulation of immune cell differentiation.
Keywords: aging; immune system; inflammation; myocardial infarction; therapeutics.
Conflict of interest statement
The Authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
