

Immunotherapy in Corticotroph and Lactotroph Aggressive Tumors and Carcinomas: Two Case Reports and a Review of the Literature
- PMID: 32823651
- PMCID: PMC7563495
- DOI: 10.3390/jpm10030088
Immunotherapy in Corticotroph and Lactotroph Aggressive Tumors and Carcinomas: Two Case Reports and a Review of the Literature
Abstract
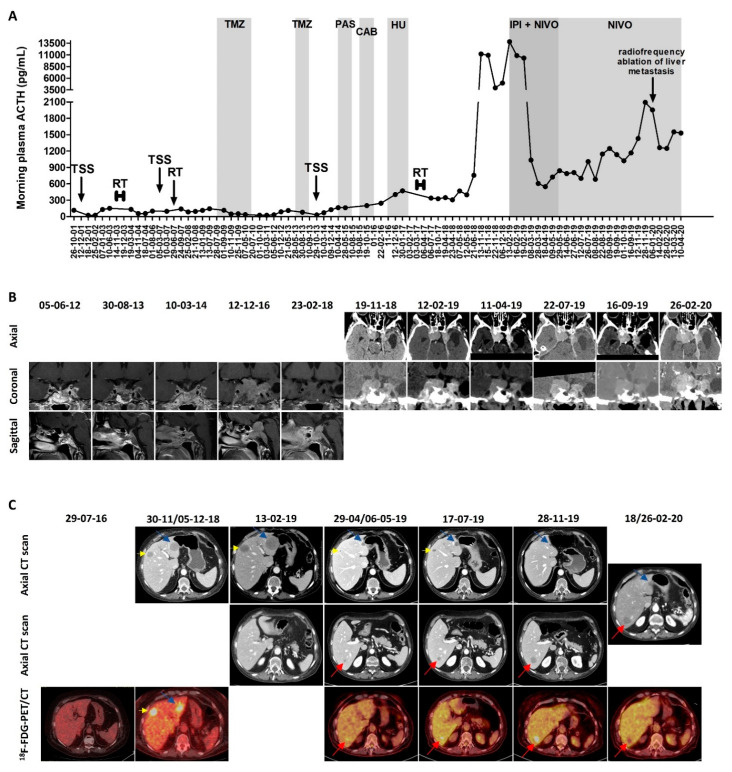
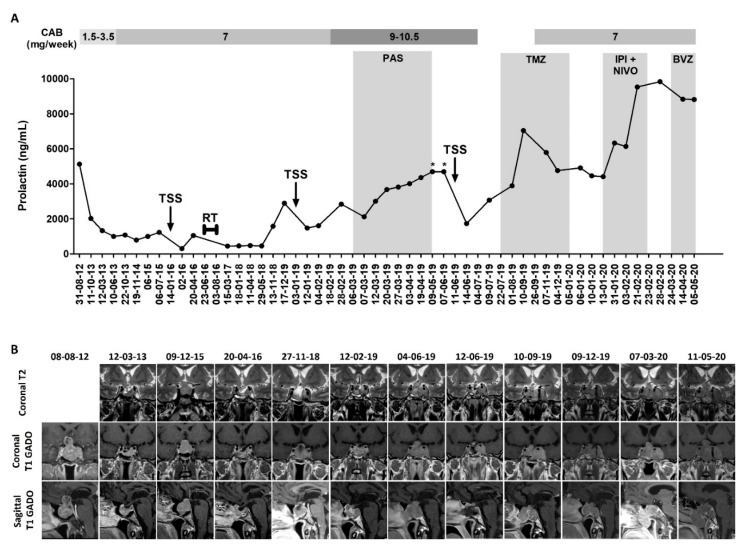
Once temozolomide has failed, no other treatment is recommended for pituitary carcinomas and aggressive pituitary tumors. Recently, the use of immune checkpoint inhibitors (ICIs) has raised hope, but so far, only one corticotroph carcinoma and one aggressive corticotroph tumor treated with immunotherapies have been reported in the literature. Here, we present two cases, one corticotroph carcinoma and one aggressive prolactinoma (the first one reported in the literature) treated with ipilimumab (1 mg/kg) and nivolumab (3 mg/kg) every three weeks, followed by maintenance treatment with nivolumab (3 mg/kg every 2 weeks) in the case of the corticotroph carcinoma, and we compare them with the two previously reported cases. Patient #1 presented a biochemical partial response (plasma ACTH decreased from 13,813 to 841 pg/mL) and dissociated radiological response to the combined ipilimumab and nivolumab-the pituitary mass decreased from 37 × 32 × 41 to 29 × 23 × 42 mm, and the pre-existing liver metastases decreased in size (the largest one from 45 to 14 mm) or disappeared, while a new 11-mm liver metastasis appeared. The maintenance nivolumab (21 cycles) resulted in a stable disease for the initial liver metastases, and in progressive disease for the newly appeared metastasis (effectively treated with radiofrequency ablation) and the pituitary mass. Patient #2 presented radiological and biochemical progressive disease after two cycles of ICIs-the pituitary mass increased from 38 × 42 × 26 to 53 × 57 × 44 mm, and the prolactin levels increased from 4410 to 9840 ng/mL. In conclusion, ICIs represent a promising therapeutic option for aggressive pituitary tumors and carcinomas. The identification of subgroups of responders will be key.
Keywords: Cushing’s disease; aggressive PitNET; aggressive pituitary adenoma; aggressive pituitary tumor; immune checkpoint inhibitors (ICIs); ipilimumab; nivolumab; pituitary carcinoma; prolactinoma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Asa S.L., Casar-Borota O., Chanson P., Delgrange E., Earls P., Ezzat S., Grossman A., Ikeda H., Inoshita N., Karavitaki N., et al. From pituitary adenoma to pituitary neuroendocrine tumor (PitNET): An International Pituitary Pathology Club proposal. Endocr. Relat. Cancer. 2017;24:C5–C8. doi: 10.1530/ERC-17-0004. - DOI - PubMed
-
- Villa C., Vasiljevic A., Jaffrain-Rea M.L., Ansorge O., Asioli S., Barresi V., Chinezu L., Gardiman M.P., Lania A., Lapshina A.M., et al. A standardised diagnostic approach to pituitary neuroendocrine tumours (PitNETs): A European Pituitary Pathology Group (EPPG) proposal. Virchows Arch. 2019;475:687–692. doi: 10.1007/s00428-019-02655-0. - DOI - PubMed
-
- Raverot G., Burman P., McCormack A., Heaney A., Petersenn S., Popovic V., Trouillas J., Dekkers O.M. European Society of Endocrinology Clinical Practice Guidelines for the management of aggressive pituitary tumours and carcinomas. Eur. J. Endocrinol. 2018;178:G1–G24. doi: 10.1530/EJE-17-0796. - DOI - PubMed
-
- Bengtsson D., Schrøder H.D., Berinder K., Maiter D., Hoybye C., Ragnarsson O., Feldt-Rasmussen U., Krogh Rasmussen Å., van der Lely A., Petersson M., et al. Tumoral MGMT content predicts survival in patients with aggressive pituitary tumors and pituitary carcinomas given treatment with temozolomide. Endocrine. 2018;62:737–739. doi: 10.1007/s12020-018-1751-9. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
