

Immune Checkpoint Inhibitors versus VEGF Targeted Therapy as Second Line Regimen in Advanced Hepatocellular Carcinoma (HCC): A Retrospective Study
- PMID: 32824968
- PMCID: PMC7563439
- DOI: 10.3390/jcm9092682
Immune Checkpoint Inhibitors versus VEGF Targeted Therapy as Second Line Regimen in Advanced Hepatocellular Carcinoma (HCC): A Retrospective Study
Abstract
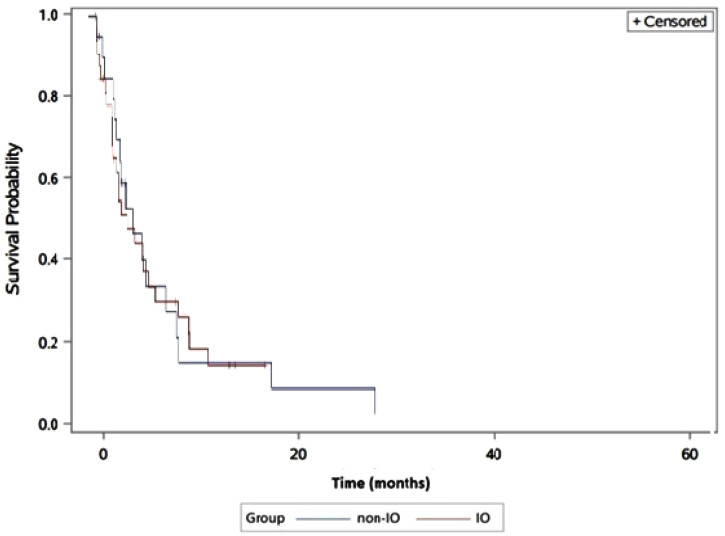
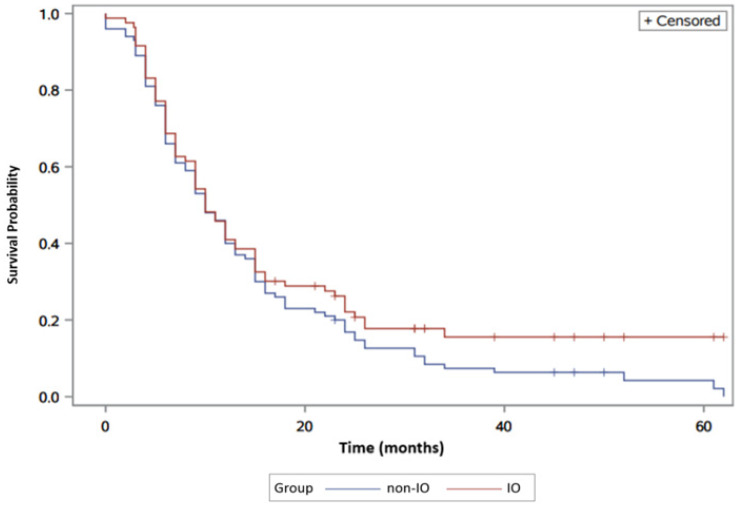
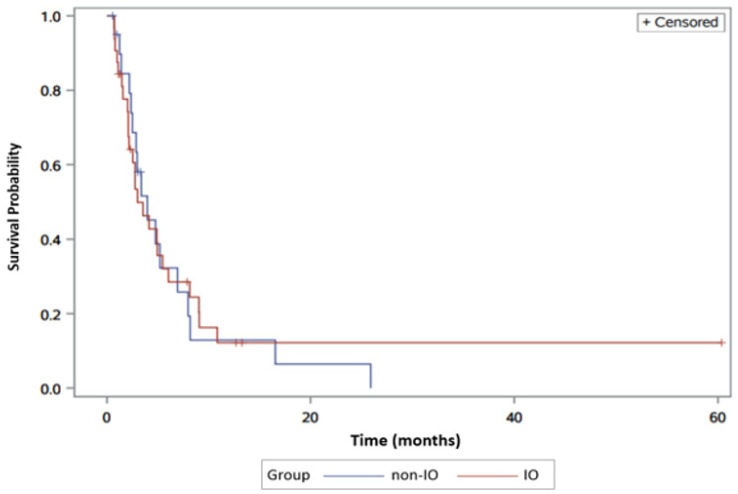
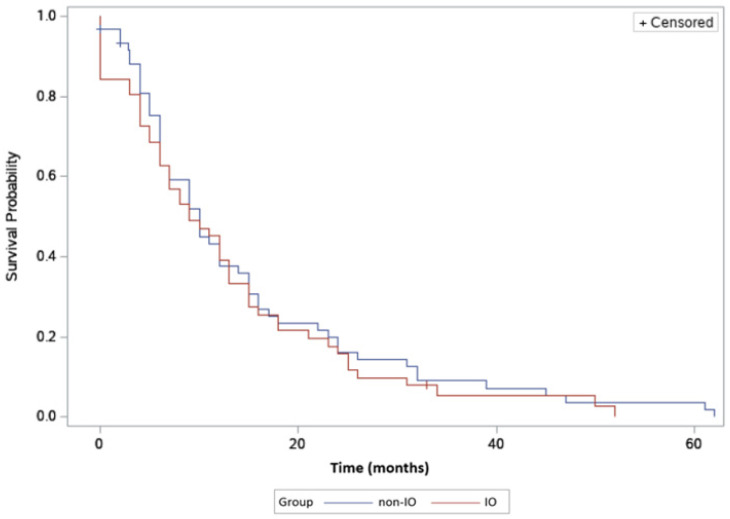
Several targeted agents including multi-tyrosine kinase inhibitors (mTKIs) and immunotherapy (IO) agents have been approved for use beyond the frontline setting in patients with advanced hepatocellular carcinoma (HCC). Due to lack of prospective head-to-head comparative trials, there is no standardized way for alternating those agents beyond frontline. Therefore, we performed a retrospective review of the Kansas University (KU) cancer registry to determine whether IO may be superior to non-IO therapy. Patients with advanced HCC were divided into two groups based on the second-line systemic regimen received (IO vs. non-IO). Progression-free survival (PFS) and overall survival (OS) were calculated under the Kaplan-Meier and Cox proportional hazards models. No statistically significant differences in PFS and OS were found, although a non-significant delayed separation in the survival curve favoring IO was identified (median PFS 3.9 months vs. 3 months; median OS 10 months vs. 10 months respectively for IO vs. non-IO). This retrospective analysis is one of the earliest and largest studies comparing second-line IO and non-IO therapies thus far reported. Future studies should aim to define specific biomarkers for response prediction and treatment optimization based on individual patient and tumor characteristics. Furthermore, combinatorial therapeutic strategies is an evolving approach showing early promising signal.
Keywords: Program Death Ligand 1; checkpoint inhibitors; hepatocellular carcinoma; immunotherapy; multi-tyrosine kinase inhibitors; targeted therapy.
Conflict of interest statement
Anwaar Saeed reports research grants (to institution) from Astrazeneca, Bristol Myers Squibb, Exelixis, Clovis, and Merck as well as advisory board/consultant fees from Bristol Myers Squibb, Astrazeneca, Merck, and Exelixis. Raed Al-Rajabi reports research grants (to institution) from Merck and Astrazeneca. Joaquina Baranda reports research grants (to institution) from Exelixis. Stephen Williamson reports research grants (to institution) from Bristol Myers Squibb and Merck. Weijing Sun reports research grants (to institution) from Merck and Astrazeneca as well as advisory board/consultant fees from Bayer. The remaining authors report no conflict of interest.
Figures
References
-
- Akinyemiju T., Abera S., Ahmed M., Alam N., Alemayohu M.A., Allen C., Al-Raddadi R., Alvis-Guzman N., Amoako Y., Artaman A., et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: Results From the Global Burden of Disease Study 2015. JAMA Oncol. 2017;3:1683–1691. doi: 10.1001/jamaoncol.2017.3055. - DOI - PMC - PubMed
-
- Kudo M., Finn R.S., Qin S., Han K.H., Ikeda K., Piscaglia F., Baron A., Park J.W., Han G., Jassem J., et al. Lenvatinib Versus Sorafenib In First-line Treatment of Patients With Unresectable Hepatocellular Carcinoma: A Randomised Phase 3 Non-inferiority Trial. Lancet. 2018;391:1163–1173. doi: 10.1016/S0140-6736(18)30207-1. - DOI - PubMed
LinkOut - more resources
Full Text Sources
