

Efficacy of Rituximab and Plasma Exchange in Antineutrophil Cytoplasmic Antibody-Associated Vasculitis with Severe Kidney Disease
- PMID: 32826324
- PMCID: PMC7608964
- DOI: 10.1681/ASN.2019111197
Efficacy of Rituximab and Plasma Exchange in Antineutrophil Cytoplasmic Antibody-Associated Vasculitis with Severe Kidney Disease
Abstract
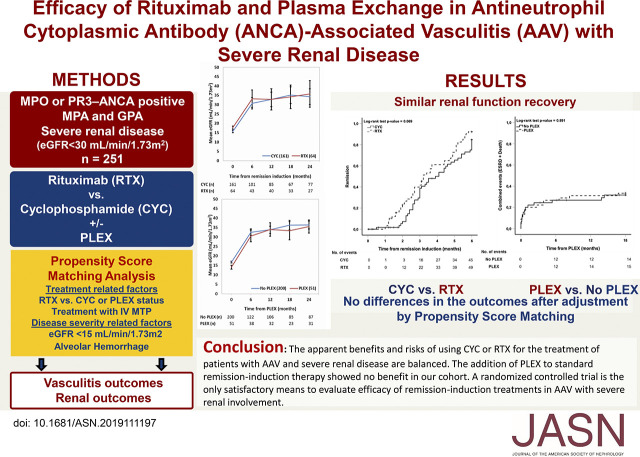
Background: Treatment of patients with ANCA-associated vasculitis (AAV) and severe renal involvement is not established. We describe outcomes in response to rituximab (RTX) versus cyclophosphamide (CYC) and plasma exchange (PLEX).
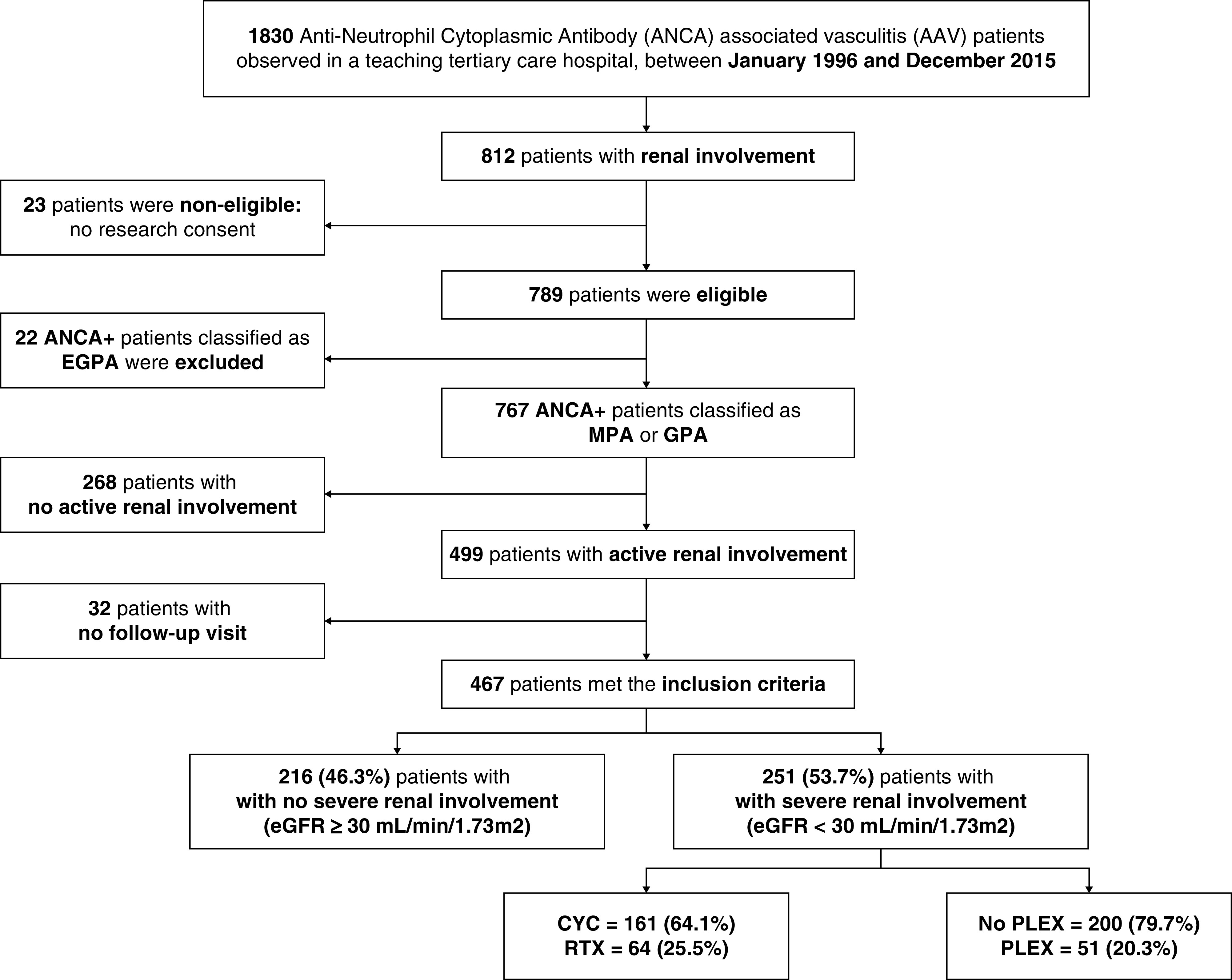
Methods: A retrospective cohort study of MPO- or PR3-ANCA-positive patients with AAV (MPA and GPA) and severe kidney disease (eGFR <30 ml/min per 1.73 m2). Remission, relapse, ESKD and death after remission-induction with CYC or RTX, with or without the use of PLEX, were compared.
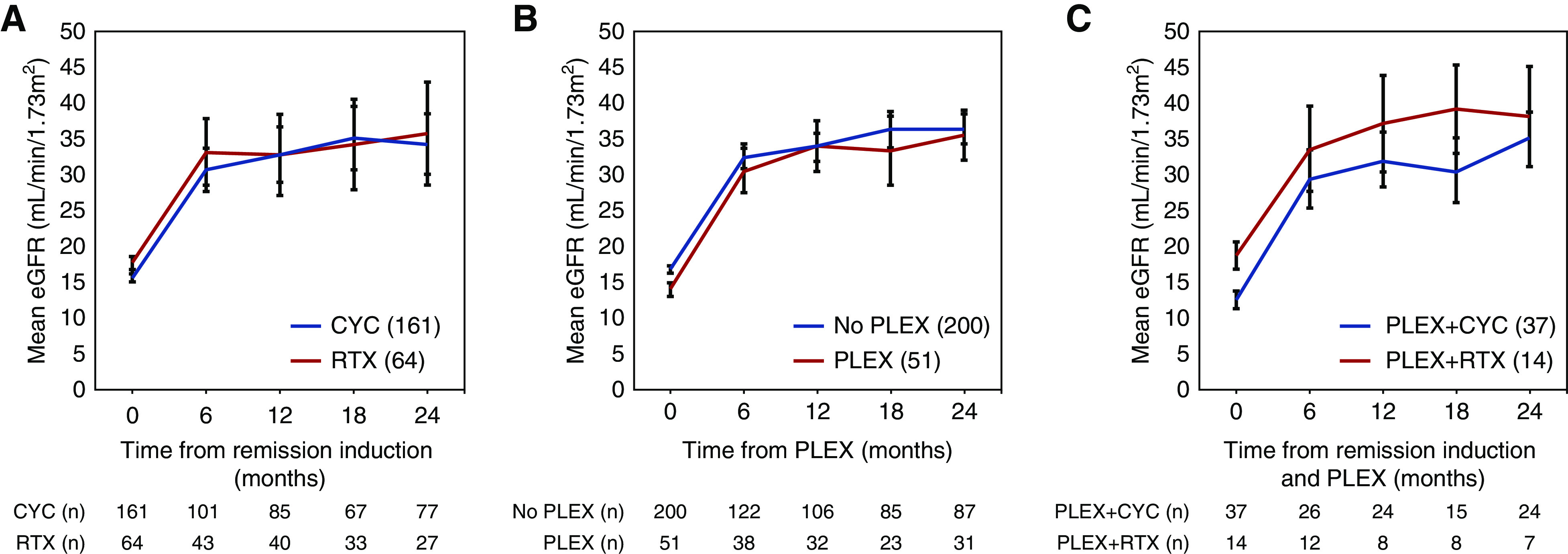
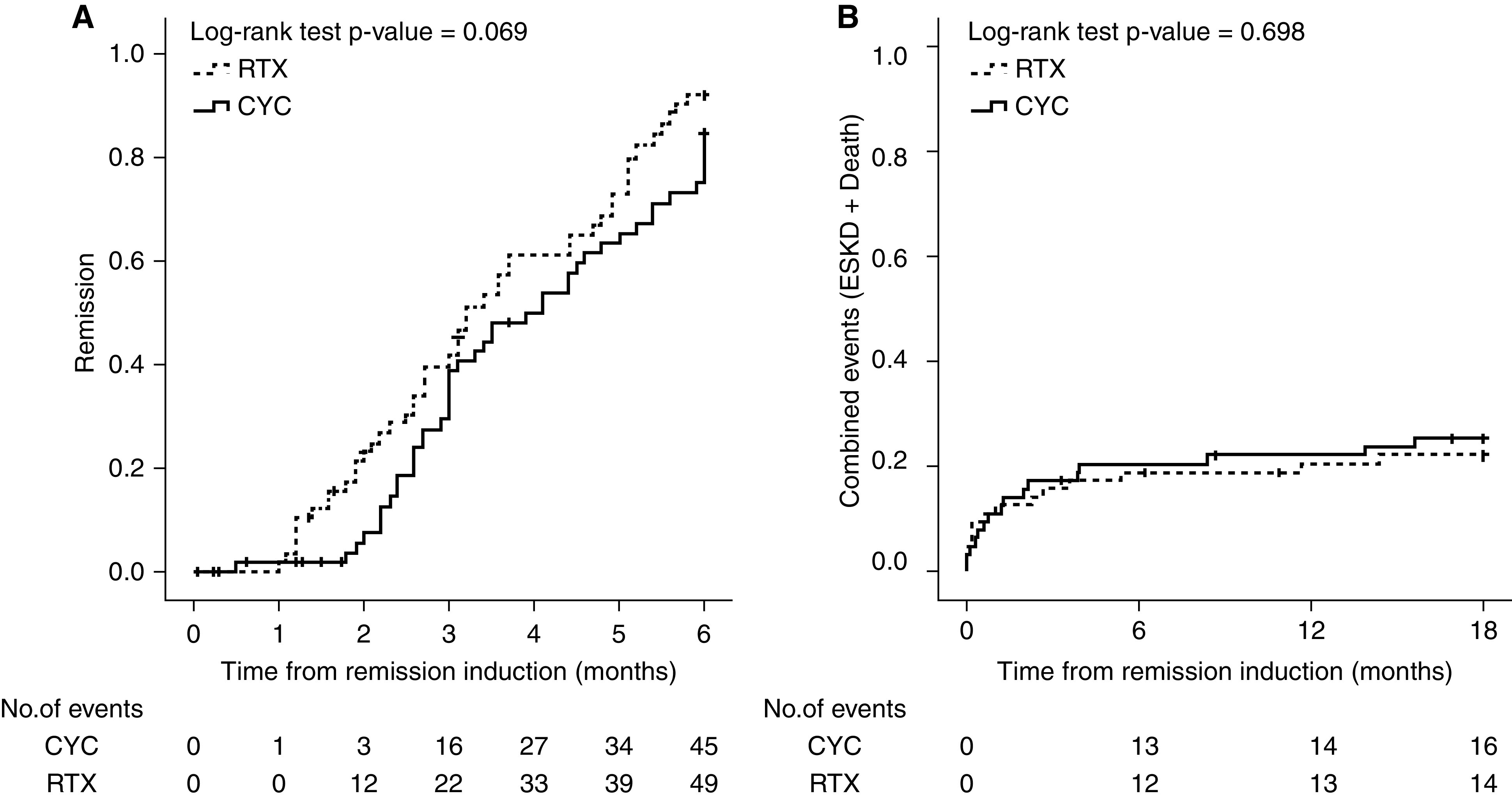
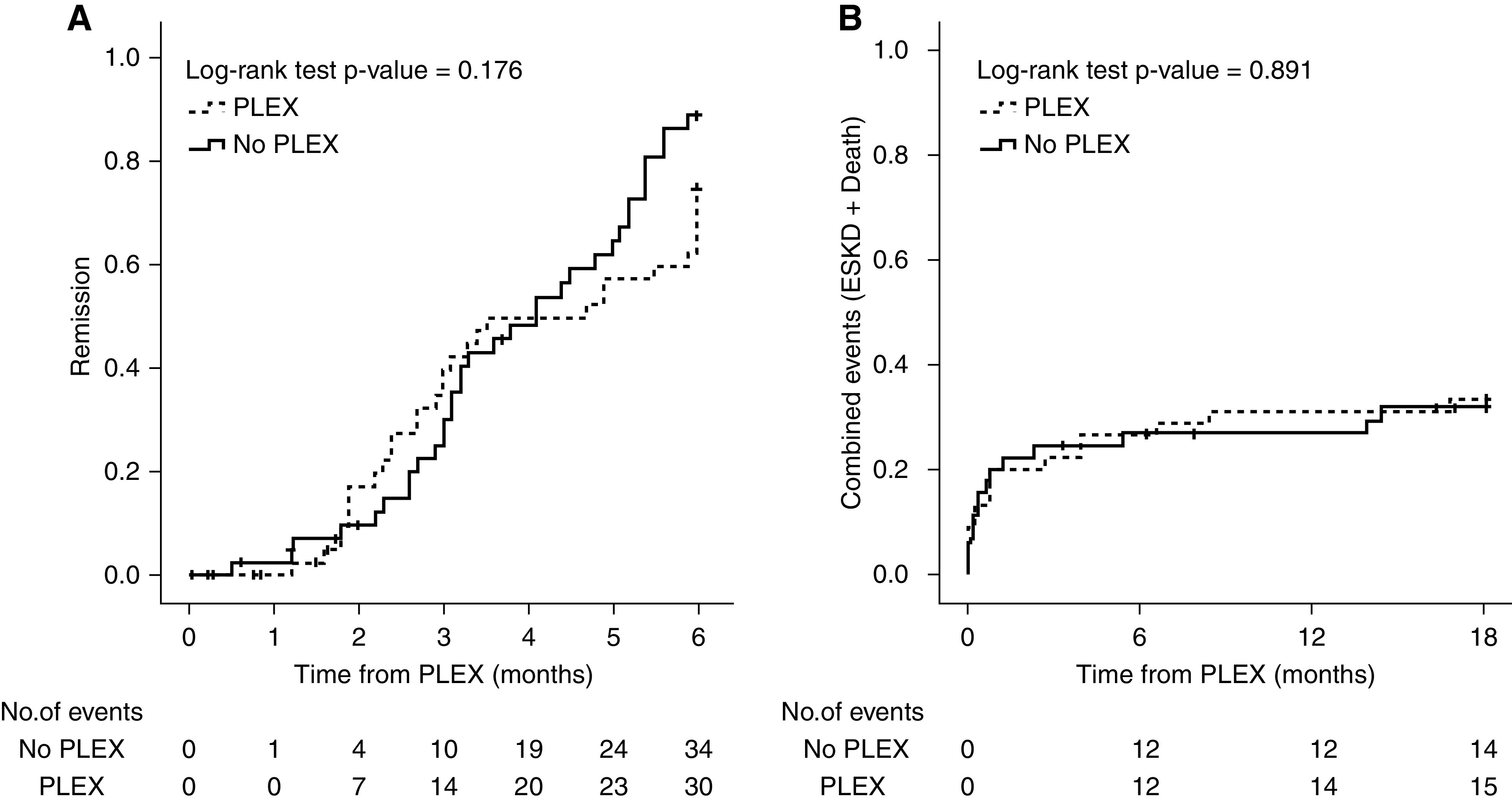
Results: Of 467 patients with active renal involvement, 251 had severe kidney disease. Patients received CYC (n=161) or RTX (n=64) for remission-induction, and 51 were also treated with PLEX. Predictors for ESKD and/or death at 18 months were eGFR <15 ml/min per 1.73 m2 at diagnosis (IRR 3.09 [95% CI 1.49 to 6.40], P=0.002), renal recovery (IRR 0.27 [95% CI 0.12 to 0.64], P=0.003) and renal remission at 6 months (IRR 0.40 [95% CI 0.18 to 0.90], P=0.027). RTX was comparable to CYC in remission-induction (BVAS/WG=0) at 6 months (IRR 1.37 [95% CI 0.91 to 2.08], P=0.132). Addition of PLEX showed no benefit on remission-induction at 6 months (IRR 0.73 [95% CI 0.44 to 1.22], P=0.230), the rate of ESKD and/or death at 18 months (IRR 1.05 [95% CI 0.51 to 2.18], P=0.891), progression to ESKD (IRR 1.06 [95% CI 0.50 to 2.25], P=0.887), and survival at 24 months (IRR 0.54 [95% CI 0.16 to 1.85], P=0.330).
Conclusions: The apparent benefits and risks of using CYC or RTX for the treatment of patients with AAV and severe kidney disease are balanced. The addition of PLEX to standard remission-induction therapy showed no benefit in our cohort. A randomized controlled trial is the only satisfactory means to evaluate efficacy of remission-induction treatments in AAV with severe renal involvement.
Keywords: ANCA; Plasmapheresis; cyclophosphamide; glomerulonephritis; rituximab.
Copyright © 2020 by the American Society of Nephrology.
Figures
Similar articles
-
Rituximab for treatment of severe renal disease in ANCA associated vasculitis.J Nephrol. 2016 Apr;29(2):195-201. doi: 10.1007/s40620-015-0208-y. Epub 2015 May 19. J Nephrol. 2016. PMID: 25986390
-
Outcomes of remission induction therapy for ANCA-associated vasculitis in the elderly.Clin Rheumatol. 2023 Sep;42(9):2427-2435. doi: 10.1007/s10067-023-06644-2. Epub 2023 May 25. Clin Rheumatol. 2023. PMID: 37225927 Free PMC article.
-
Rituximab versus cyclophosphamide for ANCA-associated vasculitis with renal involvement.J Am Soc Nephrol. 2015 Apr;26(4):976-85. doi: 10.1681/ASN.2014010046. Epub 2014 Nov 7. J Am Soc Nephrol. 2015. PMID: 25381429 Free PMC article. Clinical Trial.
-
Paediatric anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis: an update on renal management.Pediatr Nephrol. 2018 Jan;33(1):25-39. doi: 10.1007/s00467-016-3559-2. Epub 2017 Jan 6. Pediatr Nephrol. 2018. PMID: 28062909 Free PMC article. Review.
-
Impact of rituximab trials on the treatment of ANCA-associated vasculitis.Nephrol Dial Transplant. 2014 Jun;29(6):1151-9. doi: 10.1093/ndt/gft318. Epub 2013 Oct 14. Nephrol Dial Transplant. 2014. PMID: 24126571 Review.
Cited by
-
ANCA-Associated Vasculitis: An Update.J Clin Med. 2021 Apr 1;10(7):1446. doi: 10.3390/jcm10071446. J Clin Med. 2021. PMID: 33916214 Free PMC article. Review.
-
Efficacy and safety of low-dose rituximab as induction therapy for antineutrophil cytoplasmic antibody-associated vasculitis with renal involvement: a Chinese case series.BMC Nephrol. 2023 Feb 8;24(1):28. doi: 10.1186/s12882-023-03075-8. BMC Nephrol. 2023. PMID: 36755215 Free PMC article.
-
Meta-Analytical Accuracy of ANCA Renal Risk Score for Prediction of Renal Outcome in Patients With ANCA-Associated Glomerulonephritis.Front Med (Lausanne). 2022 Jan 6;8:736754. doi: 10.3389/fmed.2021.736754. eCollection 2021. Front Med (Lausanne). 2022. PMID: 35071256 Free PMC article.
-
Consideration of Therapeutic Plasma Exchange in Association With Inflammatory Lesions in ANCA-Associated Glomerulonephritis: A Real-World Retrospective Study From a Single Center.Front Immunol. 2021 Jun 17;12:645483. doi: 10.3389/fimmu.2021.645483. eCollection 2021. Front Immunol. 2021. PMID: 34220805 Free PMC article.
-
Antineutrophil Cytoplasmic Antibody-Associated Vasculitis with Active Kidney Involvement in the United States: 2016-2020.Glomerular Dis. 2024 Jan 10;4(1):33-42. doi: 10.1159/000536168. eCollection 2024 Jan-Dec. Glomerular Dis. 2024. PMID: 38328771 Free PMC article.
References
-
- Fauci AS, Haynes BF, Katz P, Wolff SM: Wegener’s granulomatosis: Prospective clinical and therapeutic experience with 85 patients for 21 years. Ann Intern Med 98: 76–85, 1983. - PubMed
-
- Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS, Travis WD, et al. : Wegener granulomatosis: An analysis of 158 patients. Ann Intern Med 116: 488–498, 1992. - PubMed
-
- Jennette JC: Rapidly progressive crescentic glomerulonephritis. Kidney Int 63: 1164–1177, 2003. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
