

Breast cancer survival and survival gap apportionment in sub-Saharan Africa (ABC-DO): a prospective cohort study
- PMID: 32827482
- PMCID: PMC7450275
- DOI: 10.1016/S2214-109X(20)30261-8
Breast cancer survival and survival gap apportionment in sub-Saharan Africa (ABC-DO): a prospective cohort study
Abstract
Background: Breast cancer is the second leading cause of death from cancer in women in sub-Saharan Africa, yet there are few well characterised large-scale survival studies with complete follow-up data. We aimed to provide robust survival estimates in women in this setting and apportion the survival gaps.
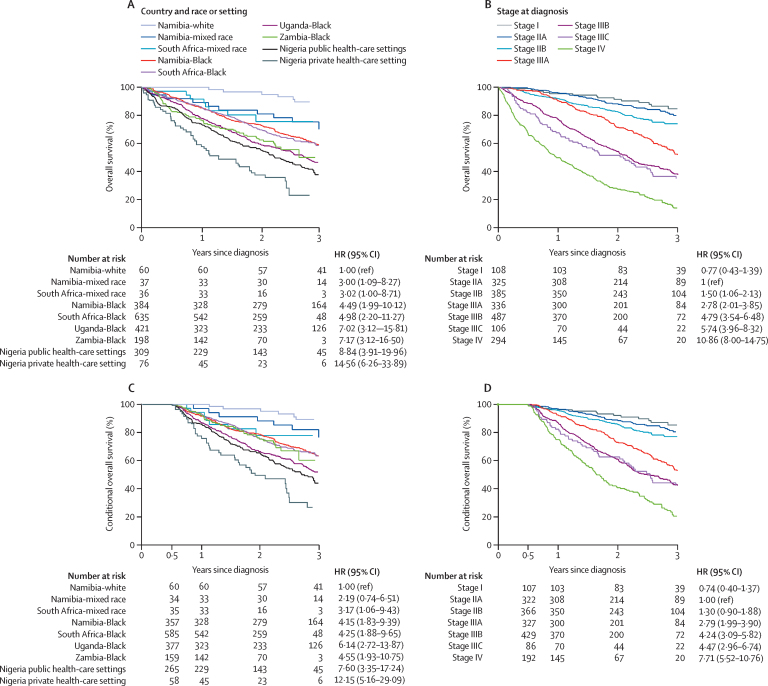
Methods: The African Breast Cancer-Disparities in Outcomes (ABC-DO) prospective cohort study was done at eight hospitals across five sub-Saharan African countries (Namibia, Nigeria, South Africa, Uganda, and Zambia). We prospectively recruited women (aged ≥18 years) who attended these hospitals with suspected breast cancer. Women were actively followed up by use of a telephone call once every 3 months, and a mobile health application was used to keep a dynamic record of follow-up calls due. We collected detailed sociodemographic, clinical, and treatment data. The primary outcome was 3-year overall survival, analysed by use of flexible proportional mortality models, and we predicted survival under scenarios of modified distributions of risk factors.
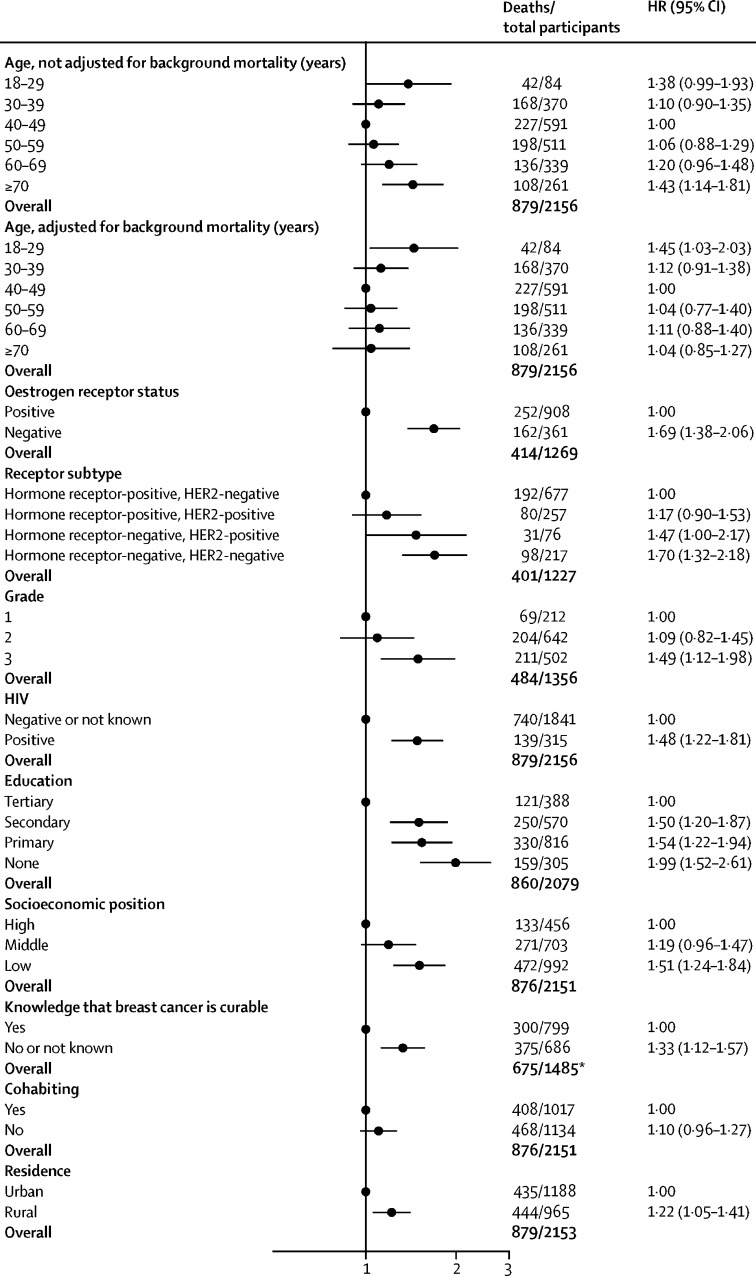
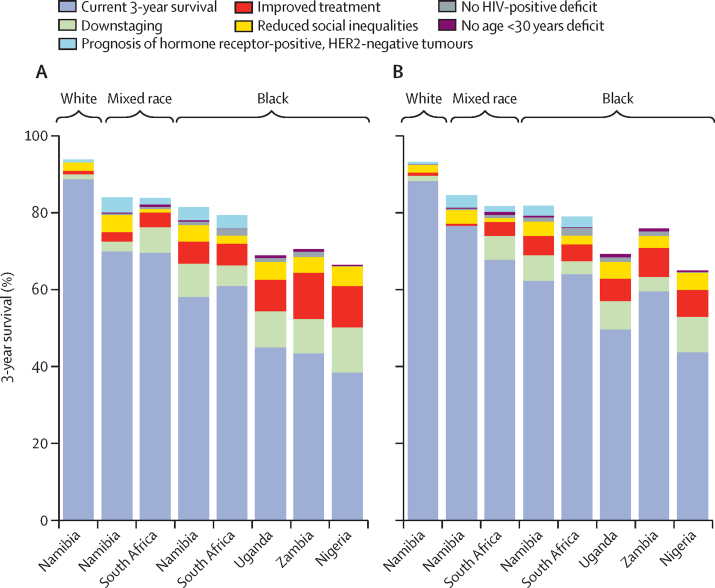
Findings: Between Sept 8, 2014, and Dec 31, 2017, 2313 women were recruited from these eight hospitals, of whom 85 did not have breast cancer. Of the remaining 2228 women with breast cancer, 58 women with previous treatment or recurrence, and 14 women from small racial groups (white and Asian women in South Africa), were excluded. Of the 2156 women analysed, 1840 (85%) were histologically confirmed, 129 (6%) were cytologically confirmed, and 187 (9%) were clinically confirmed to have breast cancer. 2156 (97%) women were followed up for up to 3 years or up to Jan 1, 2019, whichever was earlier. Up to this date, 879 (41%) of these women had died, 1118 (52%) were alive, and 159 (7%) were censored early. 3-year overall survival was 50% (95% CI 48-53), but we observed variations in 3-year survival between different races in Namibia (from 90% in white women to 56% in Black women) and in South Africa (from 76% in mixed-race women to 59% in Black women), and between different countries (44-47% in Uganda and Zambia vs 36% in Nigeria). 215 (10%) of all women had died within 6 months of diagnosis, but 3-year overall survival remained low in women who survived to this timepoint (58%). Among survival determinants, improvements in early diagnosis and treatment were predicted to contribute to the largest increases in survival, with a combined absolute increase in survival of up to 22% in Nigeria, Zambia, and Uganda, when compared with the contributions of other factors (such as HIV or aggressive subtypes).
Interpretation: Large variations in breast cancer survival in sub-Saharan African countries indicate that improvements are possible. At least a third of the projected 416 000 breast cancer deaths that will occur in this region in the next decade could be prevented through achievable downstaging and improvements in treatment. Improving survival in socially disadvantaged women warrants special attention.
Funding: Susan G Komen and the International Agency for Research on Cancer.
© 2020 International Agency for Research on Cancer; licensee Elsevier. This is an Open Access article published under the CC BY-NC-ND 3.0 IGO license which permits users to download and share the article for non-commercial purposes, so long as the article is reproduced in the whole without changes, and provided the original source is properly cited. This article shall not be used or reproduced in association with the promotion of commercial products, services or any entity. There should be no suggestion that IARC endorses any specific organisation, products or services. The use of the IARC logo is not permitted. This notice should be preserved along with the article's original URL.
Figures
References
-
- Ferlay J, Ervik M, Lam F. Global cancer observatory: cancer today. 2018. https://gco.iarc.fr/today/online-analysis-table?v=2018&mode=cancer&mode_...
-
- Carey LA, Perou CM, Livasy CA. Race, breast cancer subtypes, and survival in the Carolina breast cancer study. JAMA. 2006;295:2492–2502. - PubMed
-
- Sankaranarayanan R, Swaminathan R. Cancer Survival in Africa, Asia, the Caribbean and Central America. IARC Sci Publ. 2011:1–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
