

Pediatric Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Clinical Presentation, Infectivity, and Immune Responses
- PMID: 32827525
- PMCID: PMC7438214
- DOI: 10.1016/j.jpeds.2020.08.037
Pediatric Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Clinical Presentation, Infectivity, and Immune Responses
Abstract
Objectives: As schools plan for re-opening, understanding the potential role children play in the coronavirus infectious disease 2019 (COVID-19) pandemic and the factors that drive severe illness in children is critical.
Study design: Children ages 0-22 years with suspected severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection presenting to urgent care clinics or being hospitalized for confirmed/suspected SARS-CoV-2 infection or multisystem inflammatory syndrome in children (MIS-C) at Massachusetts General Hospital were offered enrollment in the Massachusetts General Hospital Pediatric COVID-19 Biorepository. Enrolled children provided nasopharyngeal, oropharyngeal, and/or blood specimens. SARS-CoV-2 viral load, ACE2 RNA levels, and serology for SARS-CoV-2 were quantified.
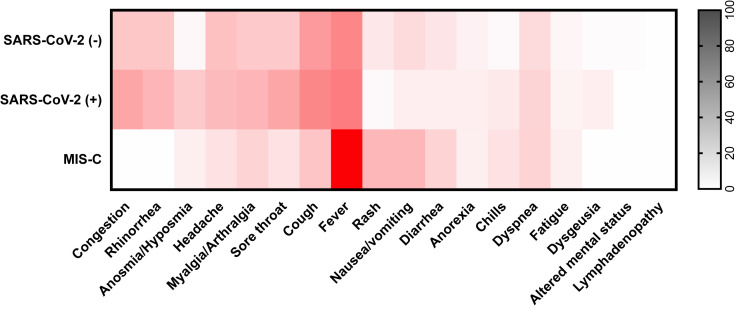
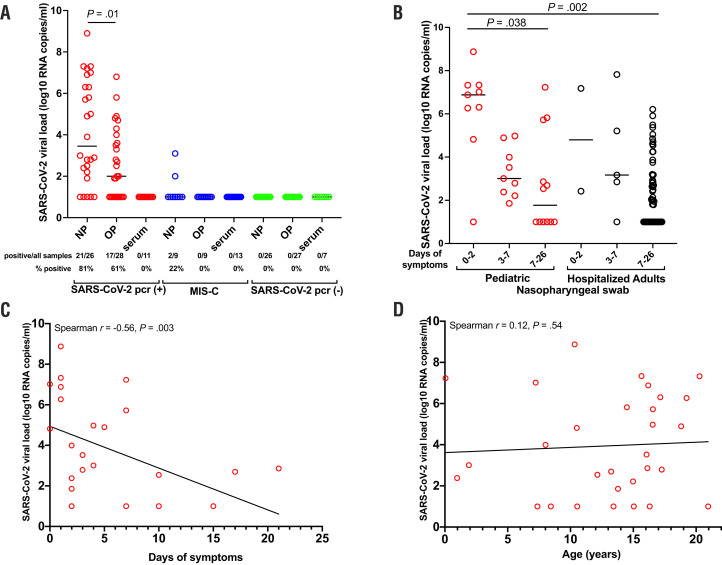
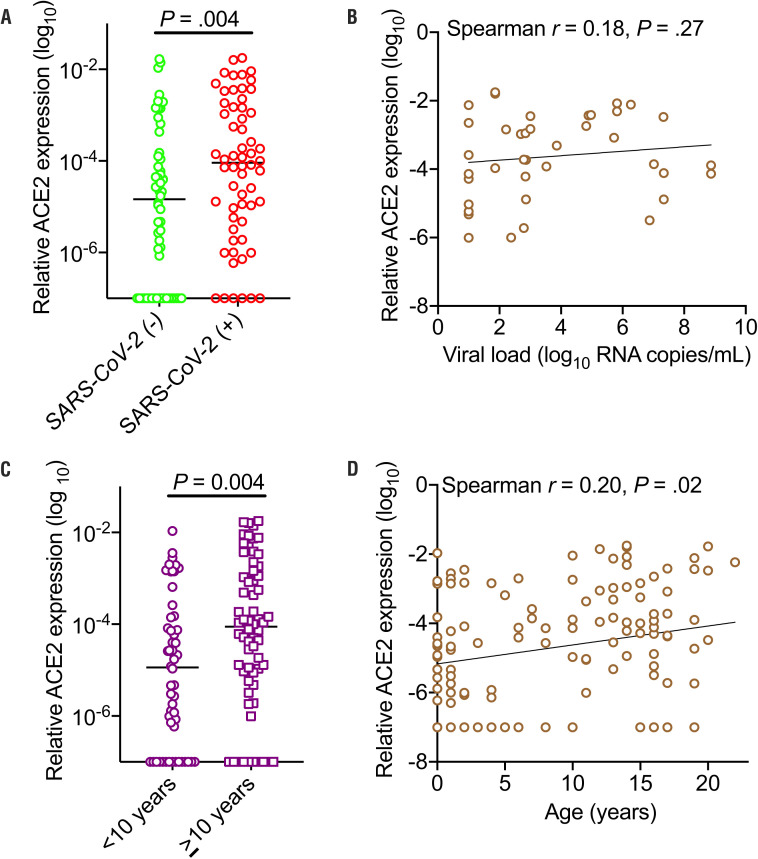
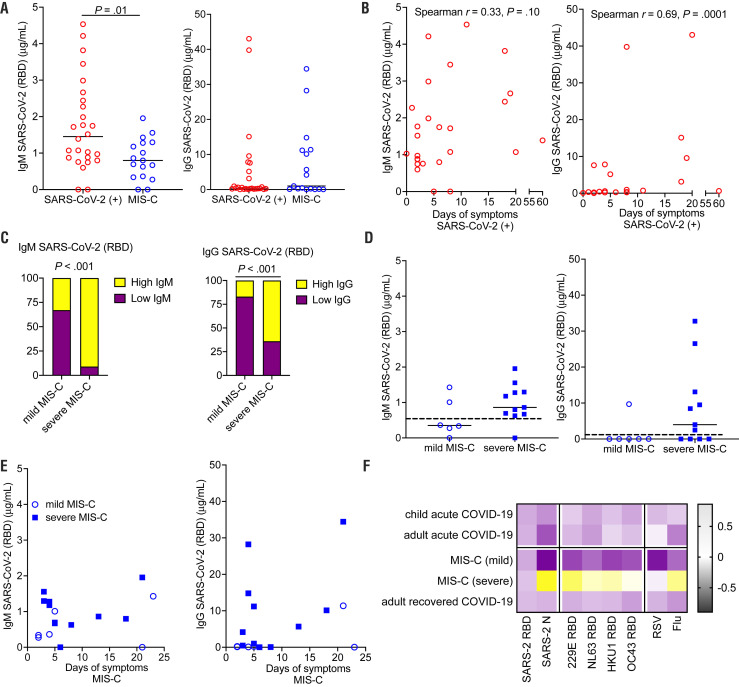
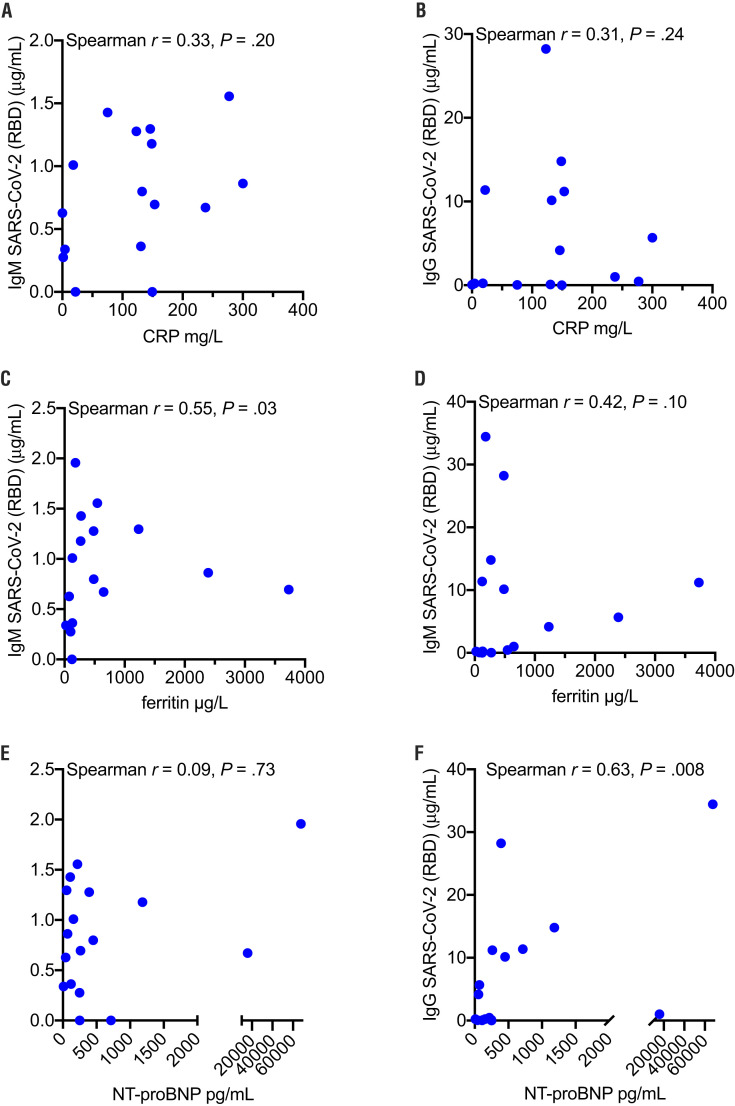
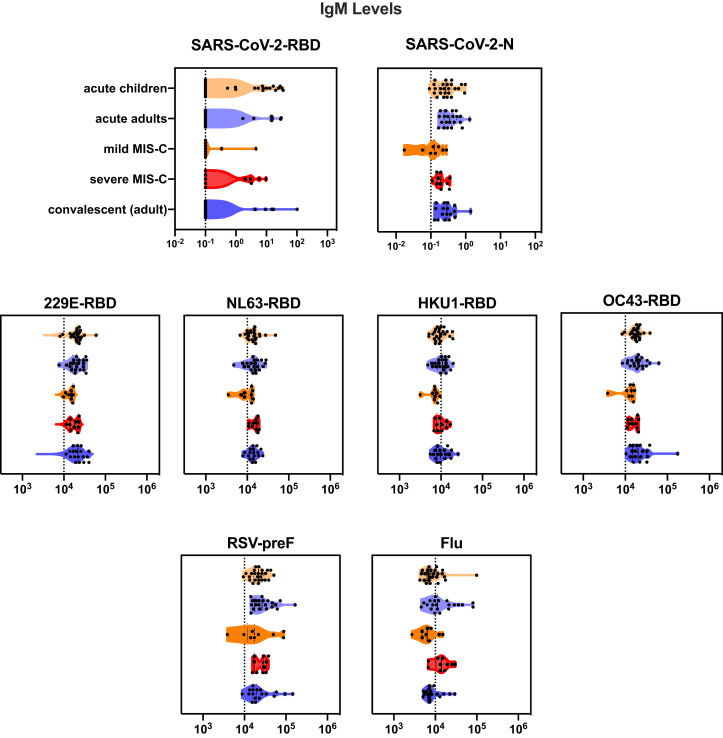
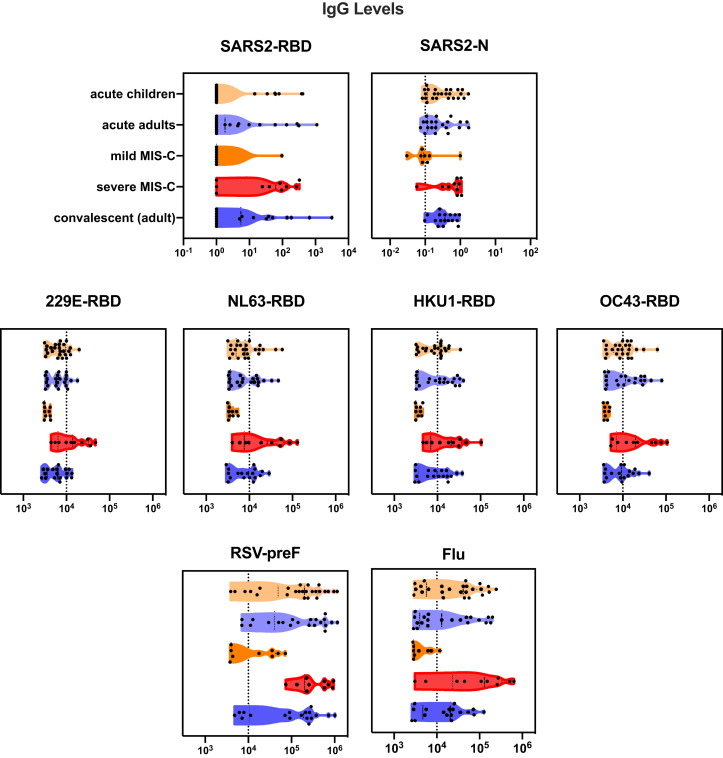
Results: A total of 192 children (mean age, 10.2 ± 7.0 years) were enrolled. Forty-nine children (26%) were diagnosed with acute SARS-CoV-2 infection; an additional 18 children (9%) met the criteria for MIS-C. Only 25 children (51%) with acute SARS-CoV-2 infection presented with fever; symptoms of SARS-CoV-2 infection, if present, were nonspecific. Nasopharyngeal viral load was highest in children in the first 2 days of symptoms, significantly higher than hospitalized adults with severe disease (P = .002). Age did not impact viral load, but younger children had lower angiotensin-converting enzyme 2 expression (P = .004). Immunoglobulin M (IgM) and Immunoglobulin G (IgG) to the receptor binding domain of the SARS-CoV-2 spike protein were increased in severe MIS-C (P < .001), with dysregulated humoral responses observed.
Conclusions: This study reveals that children may be a potential source of contagion in the SARS-CoV-2 pandemic despite having milder disease or a lack of symptoms; immune dysregulation is implicated in severe postinfectious MIS-C.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Comment regarding pediatric severe acute respiratory syndrome coronavirus 2: clinical presentation, infectivity, and immune responses.J Pediatr. 2021 Jan;228:319-320. doi: 10.1016/j.jpeds.2020.09.034. Epub 2020 Sep 18. J Pediatr. 2021. PMID: 32956699 Free PMC article. No abstract available.
-
Reply.J Pediatr. 2021 Jan;228:317-319. doi: 10.1016/j.jpeds.2020.09.049. Epub 2020 Sep 21. J Pediatr. 2021. PMID: 32971143 Free PMC article. No abstract available.
-
You say potato, I say tomato: Reassessing severe acute respiratory syndrome coronavirus 2 viral loads in children.J Pediatr. 2021 Jan;228:316-317. doi: 10.1016/j.jpeds.2020.09.048. Epub 2020 Sep 22. J Pediatr. 2021. PMID: 32971144 Free PMC article. No abstract available.
-
Does mask use affect the quantitative severe acute respiratory syndrome coronavirus 2 load in the nasopharynx?J Pediatr. 2021 Jan;228:314. doi: 10.1016/j.jpeds.2020.09.050. Epub 2020 Sep 23. J Pediatr. 2021. PMID: 32976894 Free PMC article. No abstract available.
-
Reply.J Pediatr. 2021 Jan;228:314-315. doi: 10.1016/j.jpeds.2020.09.051. Epub 2020 Sep 23. J Pediatr. 2021. PMID: 32976896 Free PMC article. No abstract available.
-
Reply.J Pediatr. 2021 Feb;229:314. doi: 10.1016/j.jpeds.2020.09.058. Epub 2020 Sep 24. J Pediatr. 2021. PMID: 32980374 Free PMC article. No abstract available.
-
RNA is not virus.J Pediatr. 2021 Feb;229:314. doi: 10.1016/j.jpeds.2020.09.057. Epub 2020 Sep 24. J Pediatr. 2021. PMID: 32980378 Free PMC article. No abstract available.
Similar articles
-
Quantitative SARS-CoV-2 Serology in Children With Multisystem Inflammatory Syndrome (MIS-C).Pediatrics. 2020 Dec;146(6):e2020018242. doi: 10.1542/peds.2020-018242. Epub 2020 Sep 2. Pediatrics. 2020. PMID: 32879033
-
Distinct Cytokine and Chemokine Dysregulation in Hospitalized Children With Acute Coronavirus Disease 2019 and Multisystem Inflammatory Syndrome With Similar Levels of Nasopharyngeal Severe Acute Respiratory Syndrome Coronavirus 2 Shedding.J Infect Dis. 2021 Aug 16;224(4):606-615. doi: 10.1093/infdis/jiab285. J Infect Dis. 2021. PMID: 34398245 Free PMC article.
-
Establishment of a pediatric COVID-19 biorepository: unique considerations and opportunities for studying the impact of the COVID-19 pandemic on children.BMC Med Res Methodol. 2020 Sep 11;20(1):228. doi: 10.1186/s12874-020-01110-y. BMC Med Res Methodol. 2020. PMID: 32917141 Free PMC article.
-
Human and novel coronavirus infections in children: a review.Paediatr Int Child Health. 2021 Feb;41(1):36-55. doi: 10.1080/20469047.2020.1781356. Epub 2020 Jun 25. Paediatr Int Child Health. 2021. PMID: 32584199 Review.
-
Age-related differences in the immune response could contribute to determine the spectrum of severity of COVID-19.Immun Inflamm Dis. 2021 Jun;9(2):331-339. doi: 10.1002/iid3.404. Epub 2021 Feb 10. Immun Inflamm Dis. 2021. PMID: 33566457 Free PMC article. Review.
Cited by
-
Asymptomatic SARS-CoV-2-infected children attending hospital with non-COVID-19 diagnoses, March 2020-February 2021.J Infect. 2021 Aug;83(2):237-279. doi: 10.1016/j.jinf.2021.05.002. Epub 2021 May 13. J Infect. 2021. PMID: 33992689 Free PMC article. No abstract available.
-
Prevalence of Chemosensory Dysfunction in COVID-19 Patients: A Systematic Review and Meta-analysis Reveals Significant Ethnic Differences.ACS Chem Neurosci. 2020 Oct 7;11(19):2944-2961. doi: 10.1021/acschemneuro.0c00460. Epub 2020 Sep 17. ACS Chem Neurosci. 2020. PMID: 32870641 Free PMC article.
-
In the long shadow of our best intentions: Model-based assessment of the consequences of school reopening during the COVID-19 pandemic.PLoS One. 2021 Mar 25;16(3):e0248509. doi: 10.1371/journal.pone.0248509. eCollection 2021. PLoS One. 2021. PMID: 33765026 Free PMC article.
-
Routine SARS-CoV-2 vaccination for all children.Immunol Rev. 2022 Aug;309(1):90-96. doi: 10.1111/imr.13108. Epub 2022 Jul 7. Immunol Rev. 2022. PMID: 35799475 Free PMC article. Review.
-
Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality.Clin Rev Allergy Immunol. 2023 Feb;64(1):90-107. doi: 10.1007/s12016-022-08921-5. Epub 2022 Jan 19. Clin Rev Allergy Immunol. 2023. PMID: 35044620 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
