

Distinct features of calcium handling and β-adrenergic sensitivity in heart failure with preserved versus reduced ejection fraction
- PMID: 32829489
- PMCID: PMC7693093
- DOI: 10.1113/JP280425
Distinct features of calcium handling and β-adrenergic sensitivity in heart failure with preserved versus reduced ejection fraction
Abstract
Key points: Heart failure (HF), the leading cause of death in developed countries, occurs in the setting of reduced (HFrEF) or preserved (HFpEF) ejection fraction. Unlike HFrEF, there are no effective treatments for HFpEF, which accounts for ∼50% of heart failure. Abnormal intracellular calcium dynamics in cardiomyocytes have major implications for contractility and rhythm, but compared to HFrEF, very little is known about calcium cycling in HFpEF. We used rat models of HFpEF and HFrEF to reveal distinct differences in intracellular calcium regulation and excitation-contraction (EC) coupling. While HFrEF is characterized by defective EC coupling at baseline, HFpEF exhibits enhanced coupling fidelity, further aggravated by a reduction in β-adrenergic sensitivity. These differences in EC coupling and β-adrenergic sensitivity may help explain why therapies that work in HFrEF are ineffective in HFpEF.
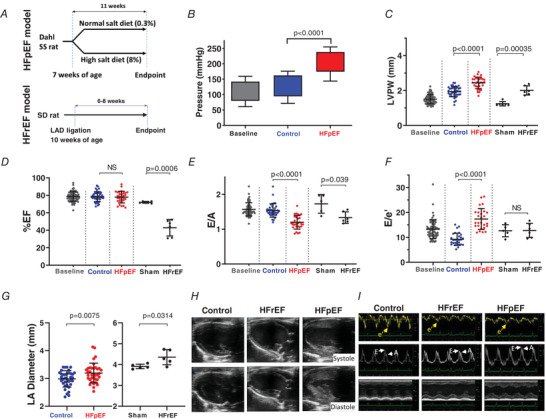
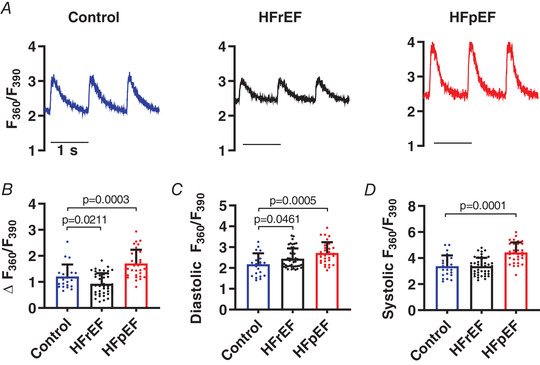
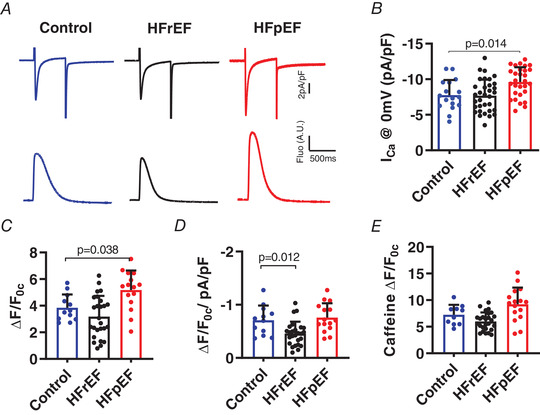
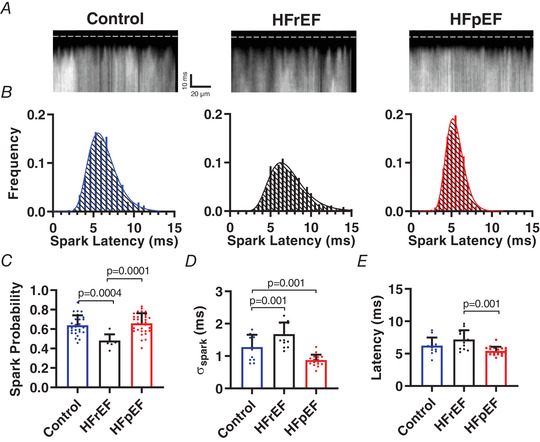
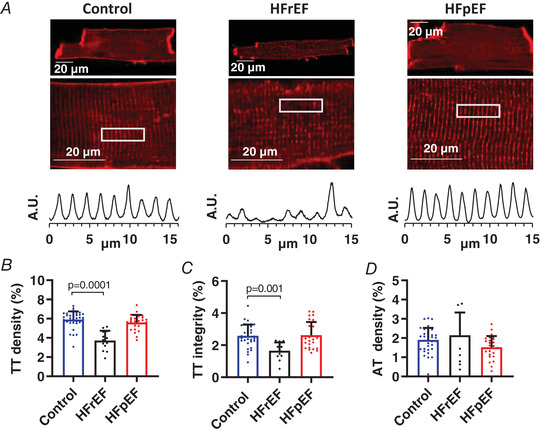
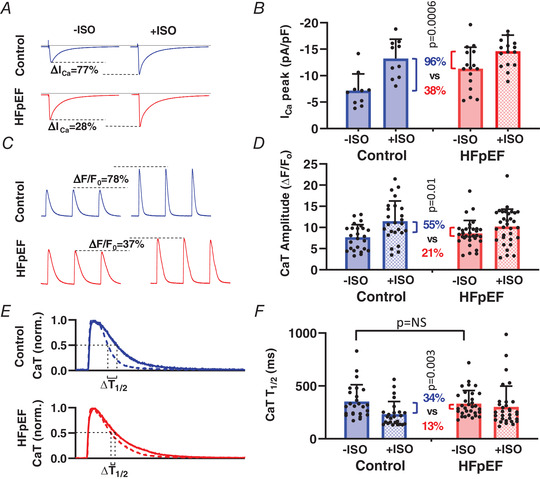
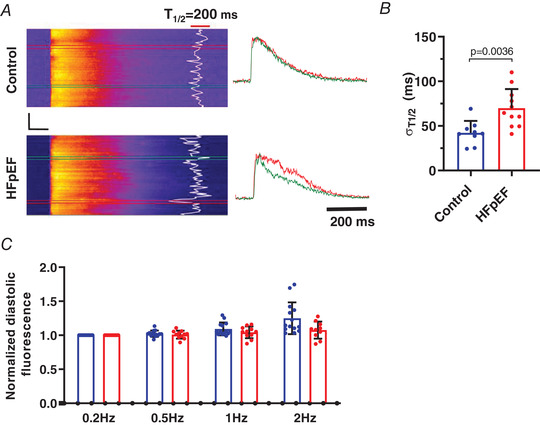
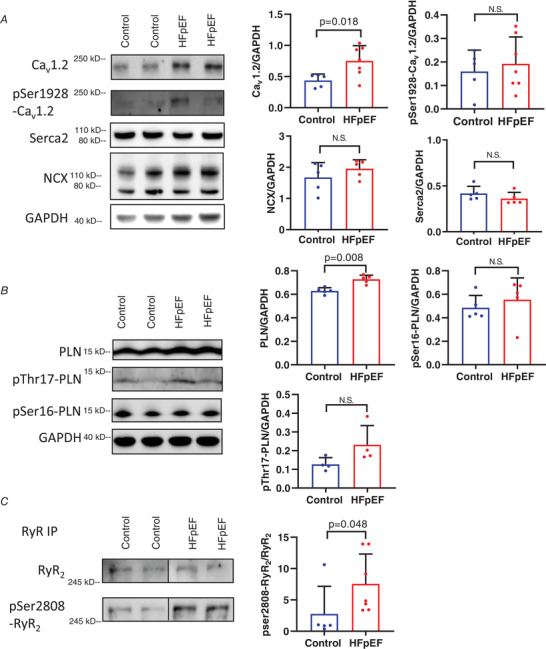
Abstract: Heart failure with reduced or preserved ejection fraction (respectively, HFrEF and HFpEF) is the leading cause of death in developed countries. Although numerous therapies improve outcomes in HFrEF, there are no effective treatments for HFpEF. We studied phenotypically verified rat models of HFrEF and HFpEF to compare excitation-contraction (EC) coupling and protein expression in these two forms of heart failure. Dahl salt-sensitive rats were fed a high-salt diet (8% NaCl) from 7 weeks of age to induce HFpEF. Impaired diastolic relaxation and preserved ejection fraction were confirmed in each animal echocardiographically, and clinical signs of heart failure were documented. To generate HFrEF, Sprague-Dawley (SD) rats underwent permanent left anterior descending coronary artery ligation which, 8-10 weeks later, led to systolic dysfunction (verified echocardiographically) and clinical signs of heart failure. Calcium (Ca2+ ) transients were measured in isolated cardiomyocytes under field stimulation or patch clamp. Ultra-high-speed laser scanning confocal imaging captured Ca2+ sparks evoked by voltage steps. Western blotting and PCR were used to assay changes in EC coupling protein and RNA expression. Cardiomyocytes from rats with HFrEF exhibited impaired EC coupling, including decreased Ca2+ transient (CaT) amplitude and defective couplon recruitment, associated with transverse (t)-tubule disruption. In stark contrast, HFpEF cardiomyocytes showed saturated EC coupling (increased ICa , high probability of couplon recruitment with greater Ca2+ release synchrony, increased CaT) and preserved t-tubule integrity. β-Adrenergic stimulation of HFpEF myocytes with isoprenaline (isoproterenol) failed to elicit robust increases in ICa or CaT and relaxation kinetics. Fundamental differences in EC coupling distinguish HFrEF from HFpEF.
Keywords: HFpEF; calcium; excitation-contraction coupling; β-adrenergic stimulation.
© 2020 The Authors. The Journal of Physiology published by John Wiley & Sons Ltd on behalf of The Physiological Society.
Figures
Comment in
-
A horse of a different colour: distinct mechanisms of HFpEF and HFrEF.J Physiol. 2020 Nov;598(22):5005-5006. doi: 10.1113/JP280691. Epub 2020 Oct 6. J Physiol. 2020. PMID: 32985684 Free PMC article. No abstract available.
-
Distinguishing HF with reduced and preserved ejection fraction at the level of individual cardiomyocytes: implications for therapeutic development.J Physiol. 2021 Feb;599(4):1027-1029. doi: 10.1113/JP280739. Epub 2020 Oct 18. J Physiol. 2021. PMID: 33017063 No abstract available.
-
New insights into heart failure during this challenging time.J Physiol. 2021 Jul;599(13):3263-3265. doi: 10.1113/JP281300. Epub 2021 Jun 1. J Physiol. 2021. PMID: 33963562 No abstract available.
References
-
- Cain BS, Meldrum DR, Joo KS, Wang JF, Meng X, Cleveland JC Jr, Banerjee A & Harken AH (1998). Human SERCA2a levels correlate inversely with age in senescent human myocardium. J Am Coll Cardiol 32, 458–467. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous