

Association of treatments for acute myocardial infarction and survival for seven common comorbidity states: a nationwide cohort study
- PMID: 32829713
- PMCID: PMC7444071
- DOI: 10.1186/s12916-020-01689-5
Association of treatments for acute myocardial infarction and survival for seven common comorbidity states: a nationwide cohort study
Abstract
Background: Comorbidity is common and has a substantial negative impact on the prognosis of patients with acute myocardial infarction (AMI). Whilst receipt of guideline-indicated treatment for AMI is associated with improved prognosis, the extent to which comorbidities influence treatment provision its efficacy is unknown. Therefore, we investigated the association between treatment provision for AMI and survival for seven common comorbidities.
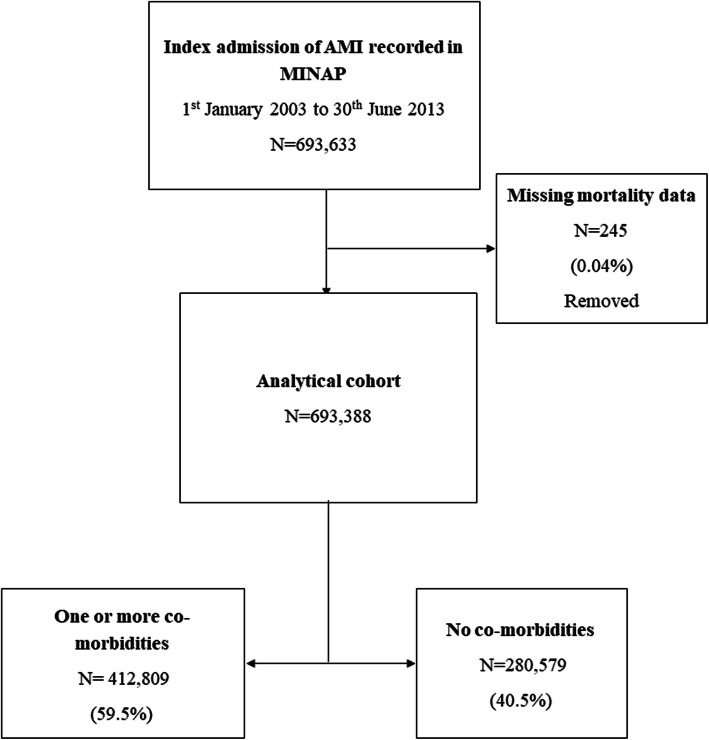
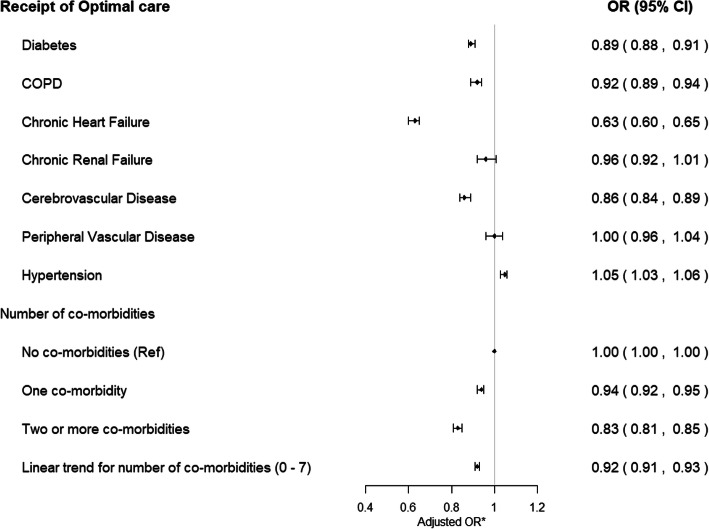
Methods: We used data of 693,388 AMI patients recorded in the Myocardial Ischaemia National Audit Project (MINAP), 2003-2013. We investigated the association between comorbidities and receipt of optimal care for AMI (receipt of all eligible guideline-indicated treatments), and the effect of receipt of optimal care for comorbid AMI patients on long-term survival using flexible parametric survival models.
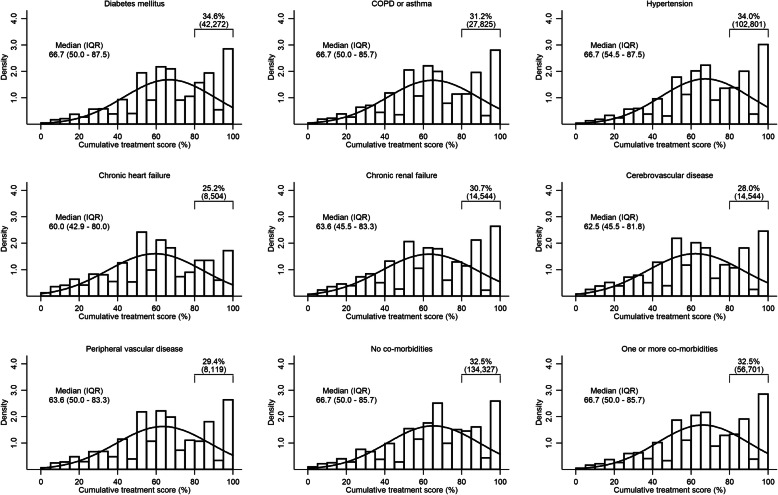
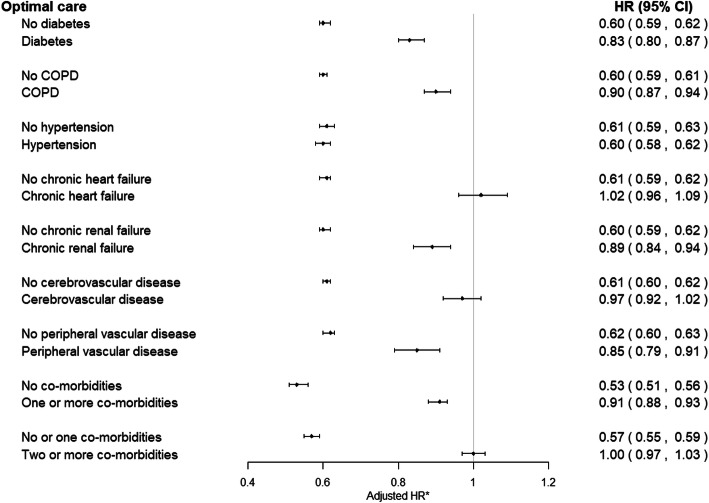
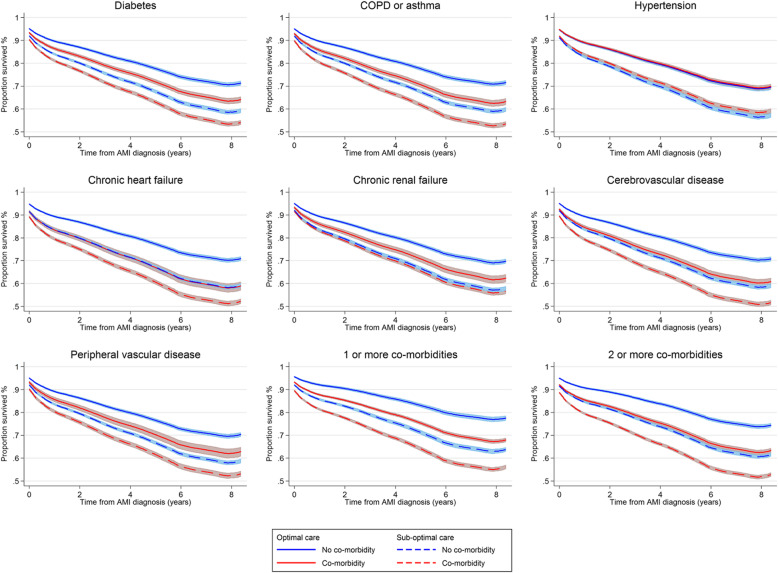
Results: A total of 412,809 [59.5%] patients with AMI had at least one comorbidity, including hypertension (302,388 [48.7%]), diabetes (122,228 [19.4%]), chronic obstructive pulmonary disease (COPD, 89,221 [14.9%]), cerebrovascular disease (51,883 [8.6%]), chronic heart failure (33,813 [5.6%]), chronic renal failure (31,029 [5.0%]) and peripheral vascular disease (27,627 [4.6%]). Receipt of optimal care was associated with greatest survival benefit for patients without comorbidities (HR 0.53, 95% CI 0.51-0.56) followed by patients with hypertension (HR 0.60, 95% CI 0.58-0.62), diabetes (HR 0.83, 95% CI 0.80-0.87), peripheral vascular disease (HR 0.85, 95% CI 0.79-0.91), renal failure (HR 0.89, 95% CI 0.84-0.94) and COPD (HR 0.90, 95% CI 0.87-0.94). For patients with heart failure and cerebrovascular disease, optimal care for AMI was not associated with improved survival.
Conclusions: Overall, guideline-indicated care was associated with improved long-term survival. However, this was not the case in AMI patients with concomitant heart failure or cerebrovascular disease. There is therefore a need for novel treatments to improve outcomes for AMI patients with pre-existing heart failure or cerebrovascular disease.
Keywords: Acute myocardial infarction; Comorbidity; Guideline care; Survival.
Conflict of interest statement
MH has received research grants from the Wellcome Trust for the submitted work; CPG has received personal fees and non-financial support from AstraZeneca; research grants and personal fees from BMS; research grants, personal fees and non-financial support from Bayer; personal fees and non-financial support from Daiichy Sankyo; and personal fees and non-financial support from Vifor Pharma, outside the submitted work. CGW reports research grants from Bristol-Myer-Squibb, outside the submitted work; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Hall M, Dondo TB, Yan AT, Mamas MA, Timmis AD, Deanfield JE, Jernberg T, Hemingway H, Fox KAA, Gale CP. Multimorbidity and survival for patients with acute myocardial infarction in England and Wales: latent class analysis of a nationwide population-based cohort. PLoS Med. 2018;15(3):e1002501. doi: 10.1371/journal.pmed.1002501. - DOI - PMC - PubMed
-
- G. B. D. Causes of Death Collaborators Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi: 10.1016/S0140-6736(18)32203-7. - DOI - PMC - PubMed
-
- Mamas MA, Fath-Ordoubadi F, Danzi GB, Spaepen E, Kwok CS, Buchan I, Peek N, de Belder MA, Ludman PF, Paunovic D, et al. Prevalence and impact of co-morbidity burden as defined by the Charlson co-morbidity index on 30-day and 1- and 5-year outcomes after coronary stent implantation (from the Nobori-2 study) Am J Cardiol. 2015;116(3):364–371. doi: 10.1016/j.amjcard.2015.04.047. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
