

Cardiac Injury Patterns and Inpatient Outcomes Among Patients Admitted With COVID-19
- PMID: 32829913
- PMCID: PMC7378523
- DOI: 10.1016/j.amjcard.2020.07.040
Cardiac Injury Patterns and Inpatient Outcomes Among Patients Admitted With COVID-19
Abstract
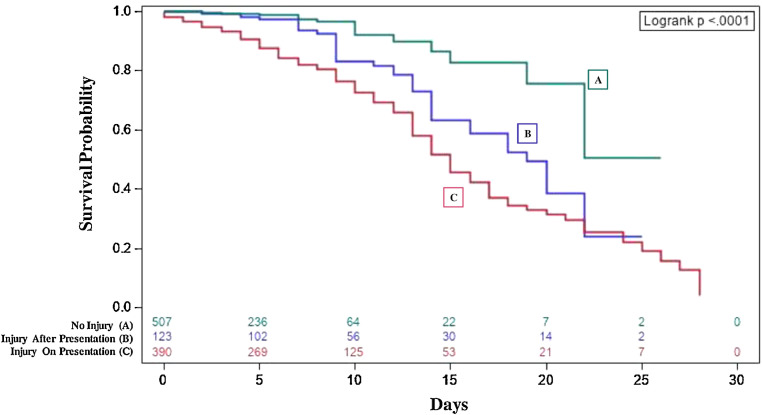
Although certain risk factors have been associated with increased morbidity and mortality in patients admitted with Coronavirus Disease 2019 (COVID-19), the impact of cardiac injury and high-sensitivity troponin-I (hs-cTnI) concentrations are not well described. In this large retrospective longitudinal cohort study, we analyzed the cases of 1,044 consecutively admitted patients with COVID-19 from March 9 until April 15. Cardiac injury was defined by hs-cTnI concentration >99th percentile. Patient characteristics, laboratory data, and outcomes were described in patients with cardiac injury and different hs-cTnI cut-offs. The primary outcome was mortality, and the secondary outcomes were length of stay, need for intensive care unit care or mechanical ventilation, and their different composites. The final analyzed cohort included 1,020 patients. The median age was 63 years, 511 (50% patients were female, and 403 (40% were white. 390 (38%) patients had cardiac injury on presentation. These patients were older (median age 70 years), had a higher cardiovascular disease burden, in addition to higher serum concentrations of inflammatory markers. They also exhibited an increased risk for our primary and secondary outcomes, with the risk increasing with higher hs-cTnI concentrations. Peak hs-cTnI concentrations continued to be significantly associated with mortality after a multivariate regression controlling for comorbid conditions, inflammatory markers, acute kidney injury, and acute respiratory distress syndrome. Within the same multivariate regression model, presenting hs-cTnI concentrations were not significantly associated with outcomes, and undetectable hs-cTnI concentrations on presentation did not completely rule out the risk for mechanical ventilation or death. In conclusion, cardiac injury was common in patients admitted with COVID-19. The extent of cardiac injury and peak hs-cTnI concentrations were associated with worse outcomes.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relations that could have appeared to influence the work reported in this study.
Figures
References
-
- Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU), Johns-Hopkins-University website. July 1, 2020.https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594.... Accessed July 1, 2020.
-
- Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, Barnaby DP, Becker LB, Chelico JD, Cohen SL, Cookingham J, Coppa K, Diefenbach MA, Dominello AJ, Duer-Hefele J, Falzon L, Gitlin J, Hajizadeh N, Harvin TG, Hirschwerk DA, Kim EJ, Kozel ZM, Marrast LM, Mogavero JN, Osorio GA, Qiu M, Zanos TP. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020;323:2052–2059. - PMC - PubMed
-
- ACC CLINICAL BULLETIN COVID-19 Clinical Guidance For the CV Care Team, American College of Cardiology website. February 07, 2020.https://www.acc.org/~/media/Non-Clinical/Files-PDFs-Excel-MS-Word-etc/20.... Accessed July 1, 2020.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
