

Chiropractic Management of Performance Related Musculoskeletal Disorder in a Career Violist
- PMID: 32830195
- PMCID: PMC7476738
- DOI: 10.12659/AJCR.923943
Chiropractic Management of Performance Related Musculoskeletal Disorder in a Career Violist
Abstract
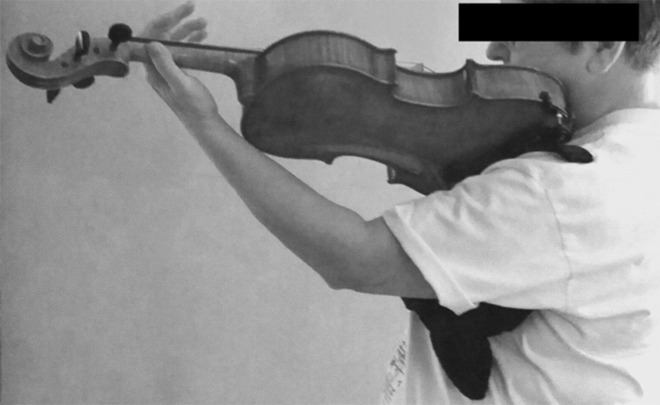
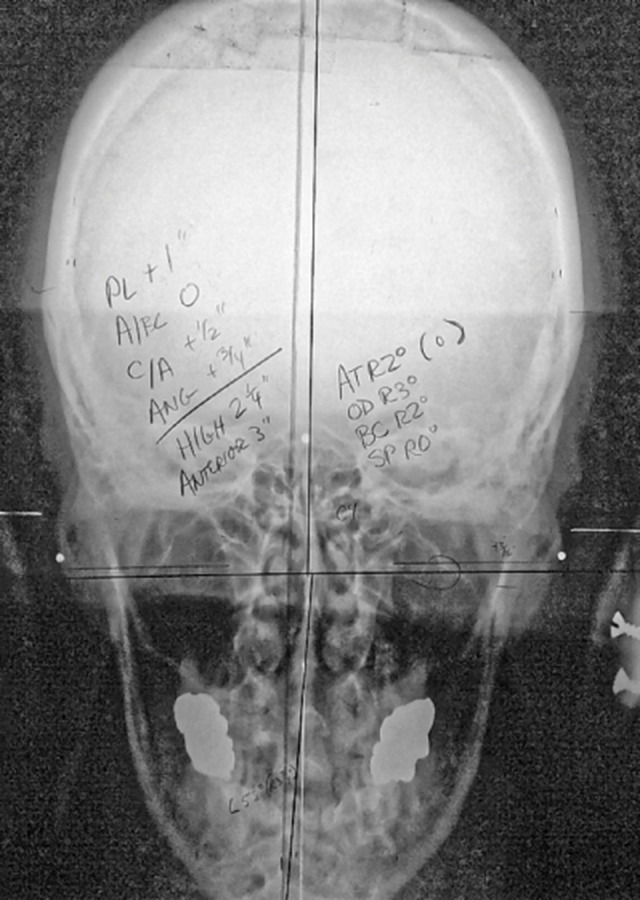
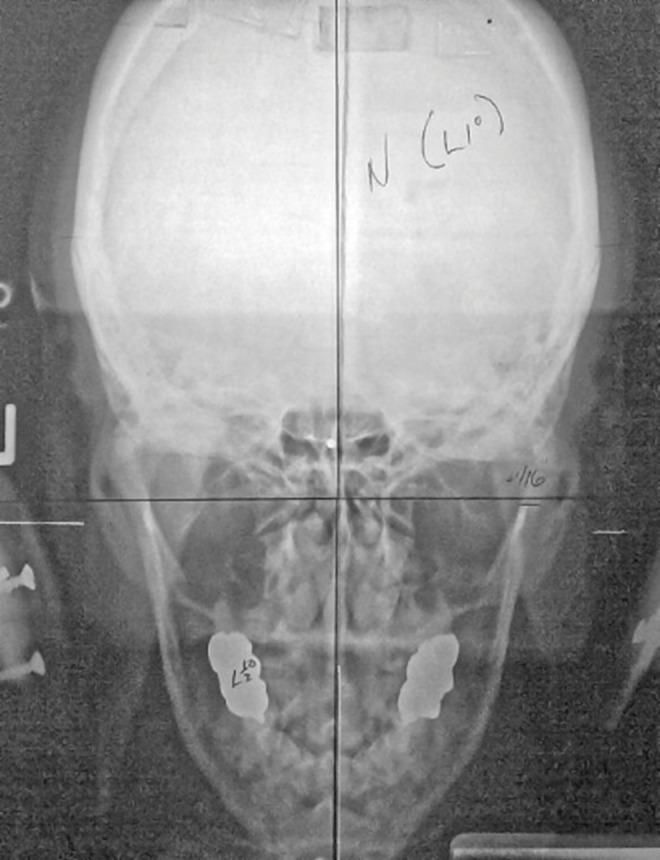
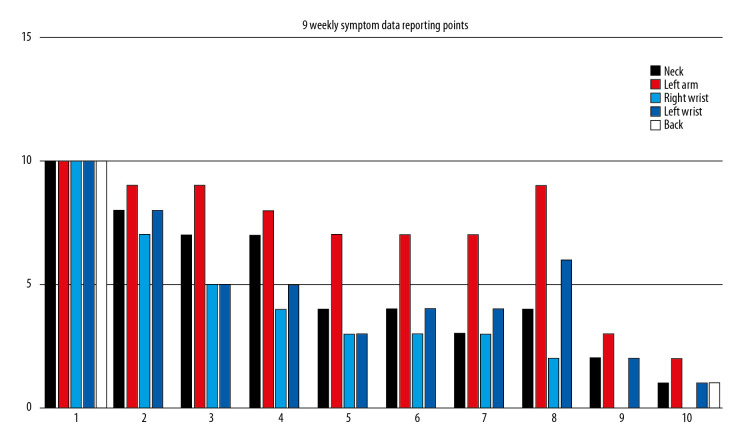
BACKGROUND Music performance is a highly stressful activity, requiring skilled neuromuscular dexterity. A lack of reported strategies for musicians suffering performance-related musculoskeletal disorders (PRMDs) exists. Papers investigating the role that postural distortions or spinal structural anomalies that could play a role in setting the stage for PRMD do not exist. The purpose of this paper was to provide a description and discussion of the use of a specialized upper cervical manual correction at the cranio-cervical junction (CCJ) to treat a violist who had disabling pain in her wrists, arms, neck, and hip. Differential diagnoses are required regarding possible confounding elements within the cervical spine. CASE REPORT After 40 years of music performance, a violist experienced severe pain while attempting to play the simplest student musical pieces. Early retirement seemed imminent. To determine appropriate chiropractic approach, the patient's clinical assessment included active range of motion, chiropractic tests, palpation, and radiographic study. Postural distortions, hypertonic muscles, joint pain, arthritis, and ponticulus posticus (PP) were noted. Upper cervical spine orthogonal radiographic series were used to develop a correction strategy. These images identified excursion of the cervical spine away from the vertical axis and C0-C1-C2 misalignments. After performing low-velocity, low-force manual correction to the CCJ, the patient experienced immediate relief of wrist pain. Over a 9-month follow-up period, the patient reported gradual decrease of pain and increased stamina while performing. Upon completing chiropractic care, the violist's career was restored. CONCLUSIONS This case supports the hypothesis that evaluating and correcting spinal structures proximal to painful extremities may represent an efficient and long-lasting solution for PRMD.
Conflict of interest statement
None.
Figures

Similar articles
-
Playing-related musculoskeletal disorders in music students-associated musculoskeletal signs.Eur J Phys Rehabil Med. 2012 Dec;48(4):625-33. Epub 2012 Nov 9. Eur J Phys Rehabil Med. 2012. PMID: 23138678
-
A musician-centered approach to management of performance-related upper musculoskeletal injuries.J Hand Ther. 2021 Apr-Jun;34(2):208-216. doi: 10.1016/j.jht.2021.04.006. Epub 2021 Apr 14. J Hand Ther. 2021. PMID: 34158229 Review.
-
Playing-Related Injuries and Posture Among Saxophonists.Med Probl Perform Art. 2019 Dec;34(4):215-221. doi: 10.21091/mppa.2019.4032. Med Probl Perform Art. 2019. PMID: 31800673
-
Ecology of musical performance as a model for evaluation and treatment of a musician with a playing related musculoskeletal disorder: A case report.J Hand Ther. 2021 Apr-Jun;34(2):330-337. doi: 10.1016/j.jht.2021.04.025. Epub 2021 May 13. J Hand Ther. 2021. PMID: 34193381
-
Line drawing analyses of static cervical X ray used in chiropractic.J Manipulative Physiol Ther. 1992 Sep;15(7):442-9. J Manipulative Physiol Ther. 1992. PMID: 1431632 Review.
References
-
- Ackermann B, Driscoll T, Kenny DT. Musculoskeletal pain and injury in professional orchestral musicians in Australia. Med Probl Perform Art. 2012;27(4):181–87. - PubMed
-
- Árnason K, Árnason Á, Briem K. Playing-related musculoskeletal disorders among Icelandic music students. Med Probl Perform Art. 2014;29(2):74–79. - PubMed
-
- Kaufman-Cohen Y, Ratzon NZ. Correlation between risk factors and musculoskeletal disorders among classical musicians. Occup Med. 2011;61(2):90–95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
