

Neurocognitive robot-assisted rehabilitation of hand function: a randomized control trial on motor recovery in subacute stroke
- PMID: 32831097
- PMCID: PMC7444058
- DOI: 10.1186/s12984-020-00746-7
Neurocognitive robot-assisted rehabilitation of hand function: a randomized control trial on motor recovery in subacute stroke
Abstract
Background: Hand function is often impaired after stroke, strongly affecting the ability to perform daily activities. Upper limb robotic devices have been developed to complement rehabilitation therapy offered to persons who suffered a stroke, but they rarely focus on the training of hand sensorimotor function. The primary goal of this study was to evaluate whether robot-assisted therapy of hand function following a neurocognitive approach (i.e., combining motor training with somatosensory and cognitive tasks) produces an equivalent decrease in upper limb motor impairment compared to dose-matched conventional neurocognitive therapy, when embedded in the rehabilitation program of inpatients in the subacute stage after stroke.
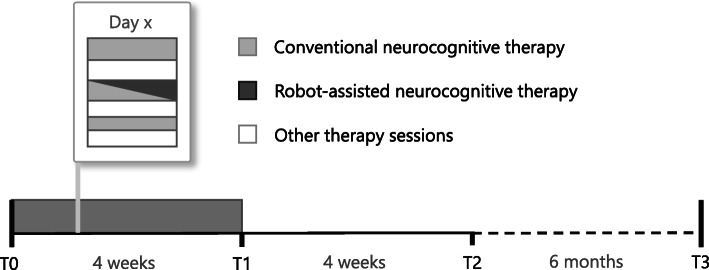
Methods: A parallel-group, randomized controlled trial was conducted on subjects with subacute stroke receiving either conventional or robot-assisted neurocognitive hand therapy using a haptic device. Therapy was provided for 15, 45-min sessions over four weeks, nested within the standard therapy program. Primary outcome was the change from baseline in the upper extremity part of the Fugl-Meyer Assessment (FMA-UE) after the intervention, which was compared between groups using equivalence testing. Secondary outcome measures included upper limb motor, sensory and cognitive assessments, delivered therapy dose, as well as questionnaires on user technology acceptance.
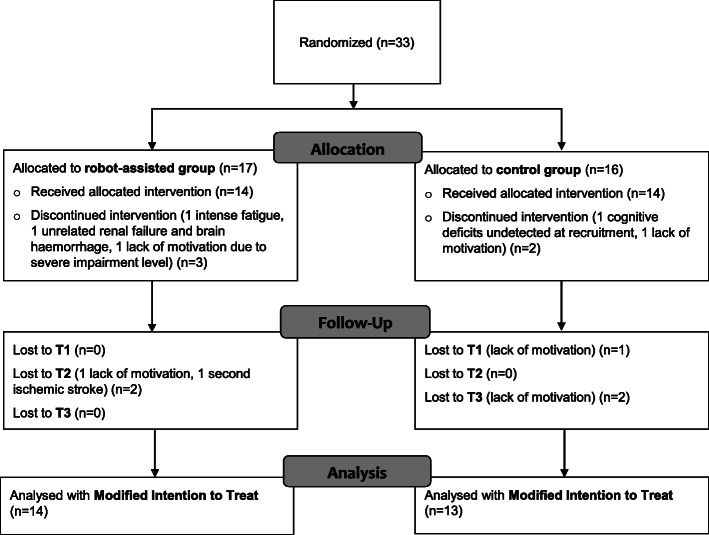
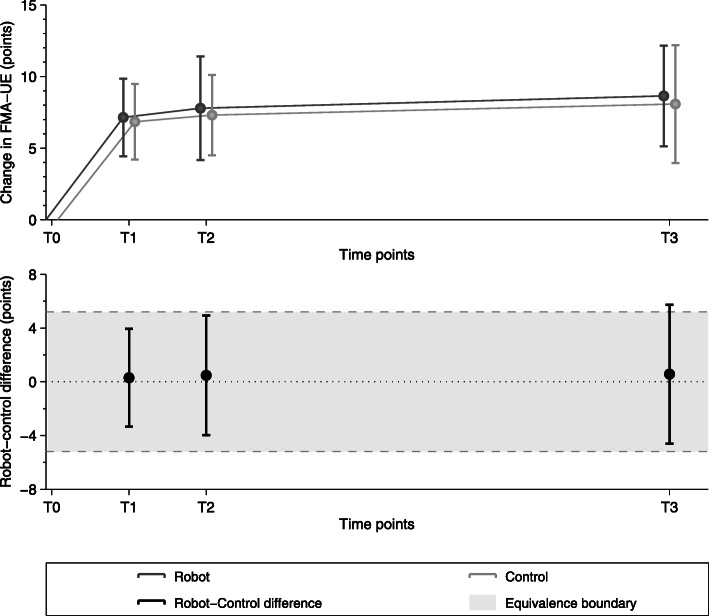
Results: Thirty-three participants with stroke were enrolled. 14 subjects in the robot-assisted and 13 subjects in the conventional therapy group completed the study. At the end of intervention, week 8 and week 32, the robot-assisted/conventional therapy group improved by 7.14/6.85, 7.79/7.31, and 8.64/8.08 points on the FMA-UE, respectively, establishing that motor recovery in the robot-assisted group is non-inferior to that in the control group.
Conclusions: Neurocognitive robot-assisted therapy of hand function allows for a non-inferior motor recovery compared to conventional dose-matched neurocognitive therapy when performed during inpatient rehabilitation in the subacute stage. This allows the early familiarization of subjects with stroke to the use of such technologies, as a first step towards minimal therapist supervision in the clinic, or directly at home after hospital discharge, to help increase the dose of hand therapy for persons with stroke.
Trial registration: EUDAMED database (CIV-13-02-009921), clinicaltrials.gov (NCT02096445). Registered 26 March 2014 - Retrospectively registered, https://clinicaltrials.gov/ct2/show/NCT02096445.
Keywords: Hand; Haptics; Neurorehabilitation; Robotics; Stroke.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Veerbeek JM, Langbroek-Amersfoort AC, van Wegen EE, Meskers CG, Kwakkel G. Effects of robot-assisted therapy for the upper limb after stroke: a systematic review and meta-analysis. Neurorehabil Neural Repair. 2017;31(2):107–121. - PubMed
-
- Klamroth-Marganska V, Blanco J, Campen K, Curt A, Dietz V, Ettlin T, et al. Three-dimensional, task-specific robot therapy of the arm after stroke: a multicentre, parallel-group randomised trial. Lancet Neurol. 2014;13(2):159–166. - PubMed
-
- Lum PS, Burgar CG, Van der Loos M, Shor PC. MIME robotic device for upper-limb neurorehabilitation in subacute stroke subjects: a follow-up study. J Rehabil Res Dev. 2006;43(5):631. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
