

Conversational Therapy through Semi-Immersive Virtual Reality Environments for Language Recovery and Psychological Well-Being in Post Stroke Aphasia
- PMID: 32831969
- PMCID: PMC7428879
- DOI: 10.1155/2020/2846046
Conversational Therapy through Semi-Immersive Virtual Reality Environments for Language Recovery and Psychological Well-Being in Post Stroke Aphasia
Abstract
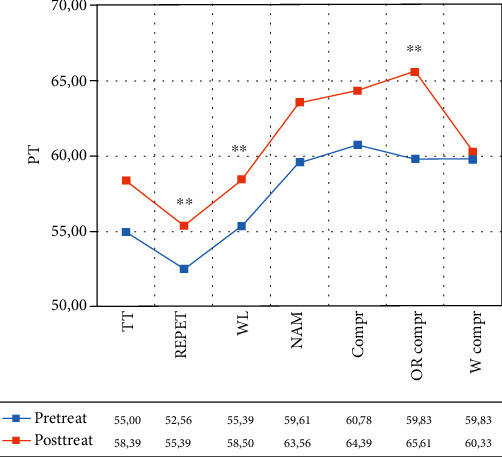
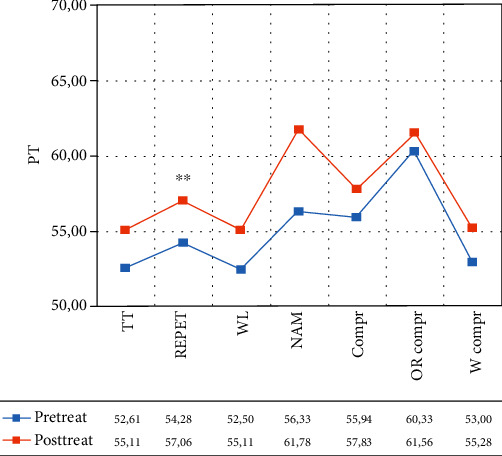
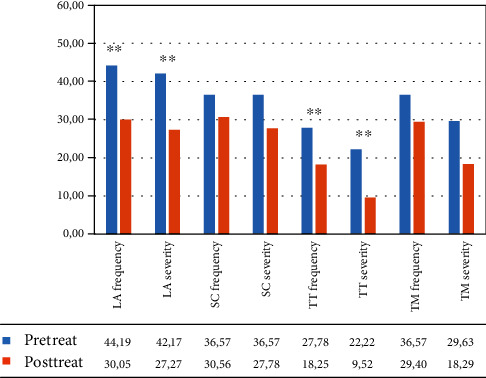
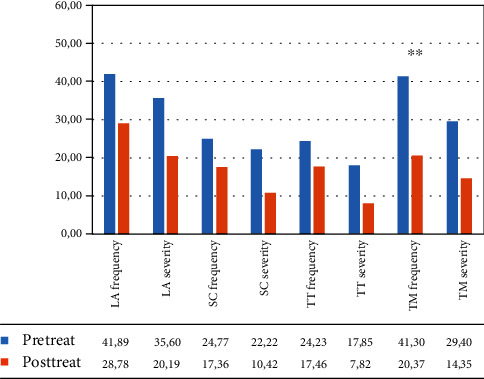
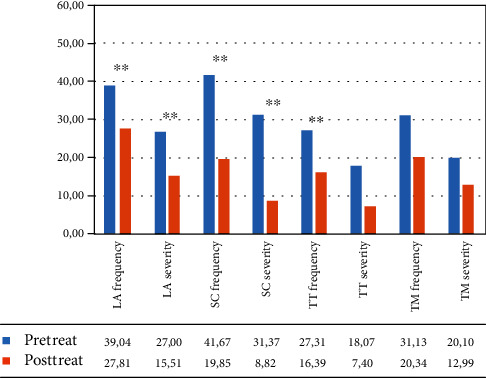
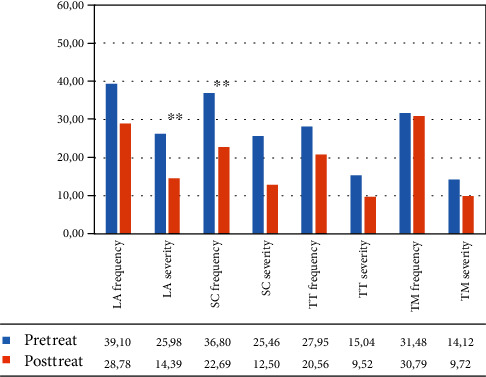
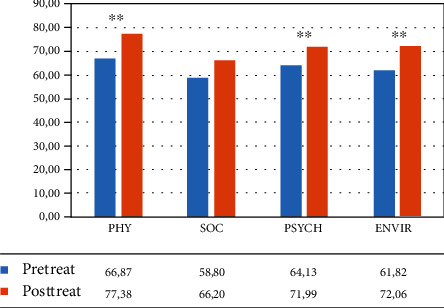
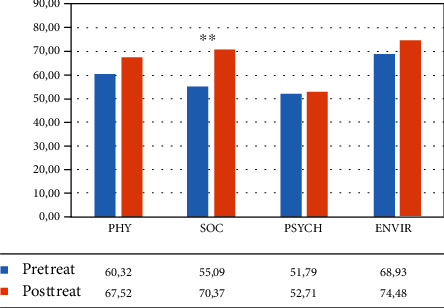
Aphasia is a highly disabling acquired language disorder generally caused by a left-lateralized brain damage. Even if traditional therapies have been shown to induce an adequate clinical improvement, a large percentage of patients are left with some degree of language impairments. Therefore, new approaches to common speech therapies are urgently needed in order to maximize the recovery from aphasia. The recent application of virtual reality (VR) to aphasia rehabilitation has already evidenced its usefulness in promoting a more pragmatically oriented treatment than conventional therapies (CT). In the present study, thirty-six chronic persons with aphasia (PWA) were randomly assigned to two groups. The VR group underwent conversational therapy during VR everyday life setting observation, while the control group was trained in a conventional setting without VR support. All patients were extensively tested through a neuropsychological battery which included not only measures for language skills and communication efficacy but also self-esteem and quality of life questionnairies. All patients were trained through a conversational approach by a speech therapist twice a week for six months (total 48 sessions). After the treatment, no significant differences among groups were found in the different measures. However, the amount of improvement in the different areas was distributed over far more cognitive and psychological aspects in the VR group than in the control group. Indeed, the within-group comparisons showed a significant enhancement in different language tasks (i.e., oral comprehension, repetition, and written language) only in the VR group. Significant gains, after the treatment, were also found, in the VR group, in different psychological dimensions (i.e., self-esteem and emotional and mood state). Given the importance of these aspects for aphasia recovery, we believe that our results add to previous evidence which points to the ecological validity and feasibility of VR treatment for language recovery and psychosocial well-being.
Copyright © 2020 A. Giachero et al.
Conflict of interest statement
The authors declare that there is no conflict of interests regarding the publication of this paper.
Figures

References
-
- Cruice M., Hill R., Worrall L., Hickson L. Conceptualising quality of life for older people with aphasia. Aphasiology. 2010;24(3):327–347. doi: 10.1080/02687030802565849. - DOI
