

Understanding Diabetic Neuropathy: Focus on Oxidative Stress
- PMID: 32832011
- PMCID: PMC7422494
- DOI: 10.1155/2020/9524635
Understanding Diabetic Neuropathy: Focus on Oxidative Stress
Abstract
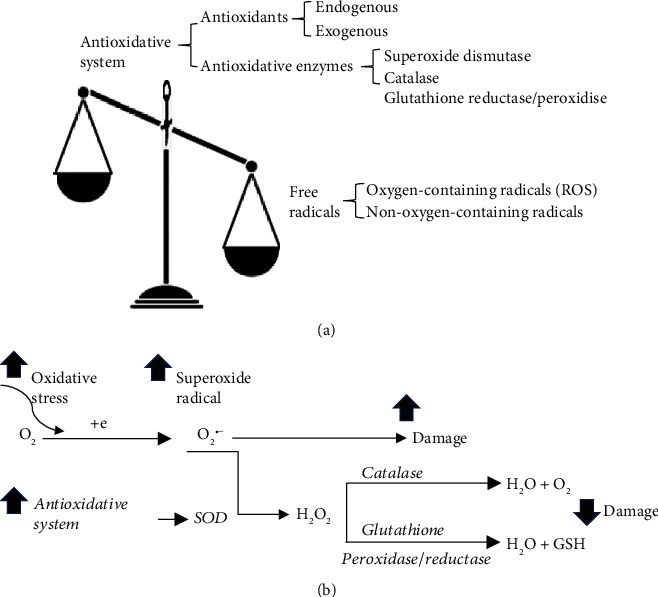
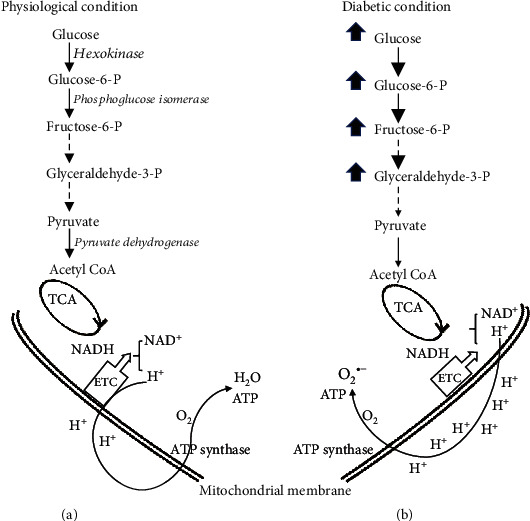
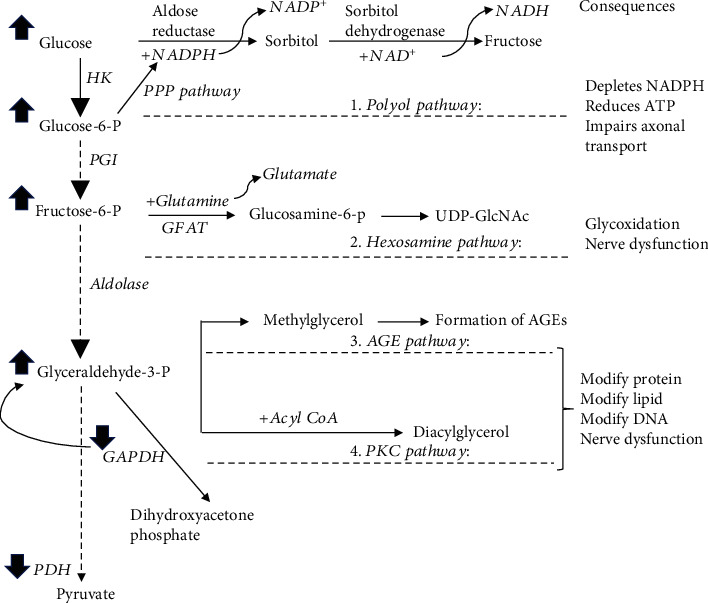
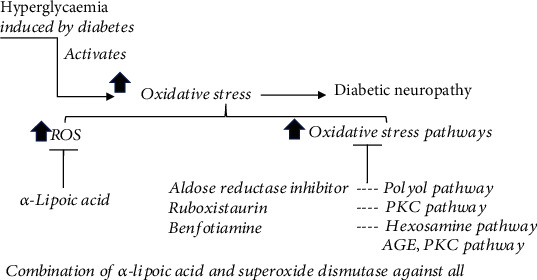
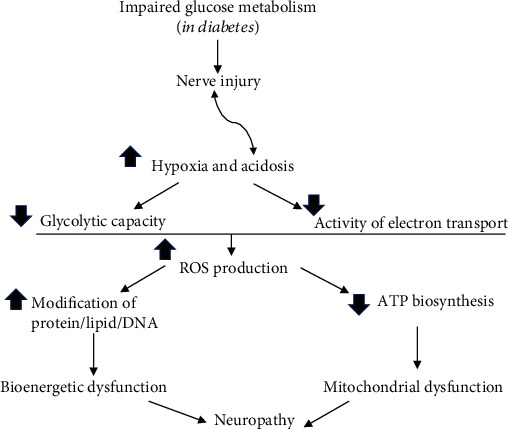
Diabetic neuropathy is one of the clinical syndromes characterized by pain and substantial morbidity primarily due to a lesion of the somatosensory nervous system. The burden of diabetic neuropathy is related not only to the complexity of diabetes but also to the poor outcomes and difficult treatment options. There is no specific treatment for diabetic neuropathy other than glycemic control and diligent foot care. Although various metabolic pathways are impaired in diabetic neuropathy, enhanced cellular oxidative stress is proposed as a common initiator. A mechanism-based treatment of diabetic neuropathy is challenging; a better understanding of the pathophysiology of diabetic neuropathy will help to develop strategies for the new and correct diagnostic procedures and personalized interventions. Thus, we review the current knowledge of the pathophysiology in diabetic neuropathy. We focus on discussing how the defects in metabolic and vascular pathways converge to enhance oxidative stress and how they produce the onset and progression of nerve injury present in diabetic neuropathy. We discuss if the mechanisms underlying neuropathy are similarly operated in type I and type II diabetes and the progression of antioxidants in treating diabetic neuropathy.
Copyright © 2020 Lei Pang et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Little A. A., Edwards J. L., Feldman E. L. Diabetic neuropathies. Practical Neurology. 2007;7(2):82–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
