

Oxygen administration in patients recovering from cardiac arrest: a narrative review
- PMID: 32832091
- PMCID: PMC7419438
- DOI: 10.1186/s40560-020-00477-w
Oxygen administration in patients recovering from cardiac arrest: a narrative review
Abstract
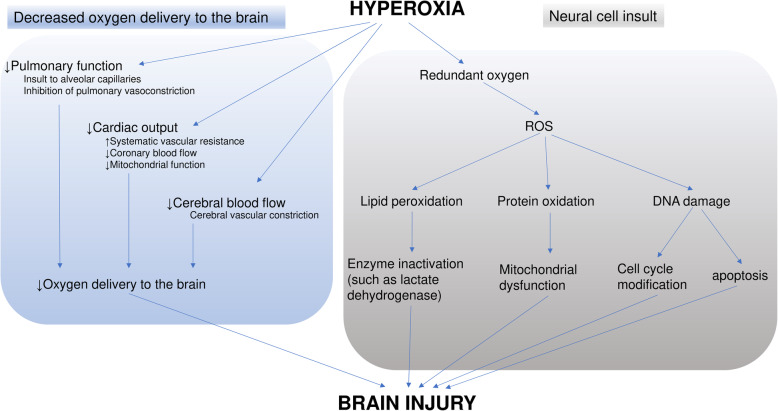
High oxygen tension in blood and/or tissue affects clinical outcomes in several diseases. Thus, the optimal target PaO2 for patients recovering from cardiac arrest (CA) has been extensively examined. Many patients develop hypoxic brain injury after the return of spontaneous circulation (ROSC); this supports the need for oxygen administration in patients after CA. Insufficient oxygen delivery due to decreased blood flow to cerebral tissue during CA results in hypoxic brain injury. By contrast, hyperoxia may increase dissolved oxygen in the blood and, subsequently, generate reactive oxygen species that are harmful to neuronal cells. This secondary brain injury is particularly concerning. Although several clinical studies demonstrated that hyperoxia during post-CA care was associated with poor neurological outcomes, considerable debate is ongoing because of inconsistent results. Potential reasons for the conflicting results include differences in the definition of hyperoxia, the timing of exposure to hyperoxia, and PaO2 values used in analyses. Despite the conflicts, exposure to PaO2 > 300 mmHg through administration of unnecessary oxygen should be avoided because no obvious benefit has been demonstrated. The feasibility of titrating oxygen administration by targeting SpO2 at approximately 94% in patients recovering from CA has been demonstrated in pilot randomized controlled trials (RCTs). Such protocols should be further examined.
Keywords: Cardiac arrest; Hyperoxia; Hypoxic brain injury; Oxygen; Post cardia arrest syndrome.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures
Similar articles
-
Randomized Trial of 21% versus 100% Oxygen during Chest Compressions Followed by Gradual versus Abrupt Oxygen Titration after Return of Spontaneous Circulation in Neonatal Lambs.Children (Basel). 2023 Mar 17;10(3):575. doi: 10.3390/children10030575. Children (Basel). 2023. PMID: 36980132 Free PMC article.
-
Targeting low- or high-normal Carbon dioxide, Oxygen, and Mean arterial pressure After Cardiac Arrest and REsuscitation: study protocol for a randomized pilot trial.Trials. 2017 Oct 30;18(1):507. doi: 10.1186/s13063-017-2257-0. Trials. 2017. PMID: 29084585 Free PMC article. Clinical Trial.
-
Association of Arterial Oxygen Tension During In-Hospital Cardiac Arrest With Return of Spontaneous Circulation and Survival.J Intensive Care Med. 2018 Jul;33(7):407-414. doi: 10.1177/0885066616658420. Epub 2016 Jul 11. J Intensive Care Med. 2018. PMID: 27402395
-
Hyperoxia After Return of Spontaneous Circulation in Cardiac Arrest Patients.J Cardiothorac Vasc Anesth. 2022 May;36(5):1419-1428. doi: 10.1053/j.jvca.2021.03.007. Epub 2021 Mar 8. J Cardiothorac Vasc Anesth. 2022. PMID: 33875350 Review.
-
How much oxygen in adult cardiac arrest?Crit Care. 2014 Oct 7;18(5):555. doi: 10.1186/s13054-014-0555-4. Crit Care. 2014. PMID: 25636001 Free PMC article. Review.
Cited by
-
Relationship between initial red cell distribution width and ΔRDW and mortality in cardiac arrest patients.ESC Heart Fail. 2024 Feb;11(1):433-443. doi: 10.1002/ehf2.14602. Epub 2023 Nov 29. ESC Heart Fail. 2024. PMID: 38030411 Free PMC article.
-
Early restricted oxygen therapy after resuscitation from cardiac arrest (ER-OXYTRAC): protocol for a stepped-wedge cluster randomised controlled trial.BMJ Open. 2023 Sep 15;13(9):e074475. doi: 10.1136/bmjopen-2023-074475. BMJ Open. 2023. PMID: 37714682 Free PMC article.
-
Hyperoxemia during resuscitation of trauma patients and increased intensive care unit length of stay: inverse probability of treatment weighting analysis.World J Emerg Surg. 2021 Apr 29;16(1):19. doi: 10.1186/s13017-021-00363-2. World J Emerg Surg. 2021. PMID: 33926507 Free PMC article.
-
Multifaceted functions of Drp1 in hypoxia/ischemia-induced mitochondrial quality imbalance: from regulatory mechanism to targeted therapeutic strategy.Mil Med Res. 2023 Oct 13;10(1):46. doi: 10.1186/s40779-023-00482-8. Mil Med Res. 2023. PMID: 37833768 Free PMC article. Review.
-
Hyperoxia for accidental hypothermia and increased mortality: a post-hoc analysis of a multicenter prospective observational study.Crit Care. 2023 Apr 1;27(1):131. doi: 10.1186/s13054-023-04407-8. Crit Care. 2023. PMID: 37005646 Free PMC article.
References
-
- Laver S, Farrow C, Turner D, Nolan J. Mode of death after admission to an intensive care unit following cardiac arrest. Intensive Care Med. 2004;30:2126–2128. - PubMed
-
- Nolan JP, Neumar RW, Adrie C, Aibiki M, Berg RA, Böttiger BW, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Stroke. Resuscitation. 2008;79:350–379. - PubMed
-
- Negovsky VA. The second step in resuscitation--the treatment of the ‘post-resuscitation disease’. Resuscitation. 1972;1:1–7. - PubMed
-
- Sjöberg F, Singer M. The medical use of oxygen: a time for critical reappraisal. J Intern Med. 2013;274:505–528. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
