

Optical Coherence Tomography Angiography Projection Artifact Removal: Impact on Capillary Density and Interaction with Diabetic Retinopathy Severity
- PMID: 32832217
- PMCID: PMC7414622
- DOI: 10.1167/tvst.9.7.10
Optical Coherence Tomography Angiography Projection Artifact Removal: Impact on Capillary Density and Interaction with Diabetic Retinopathy Severity
Abstract
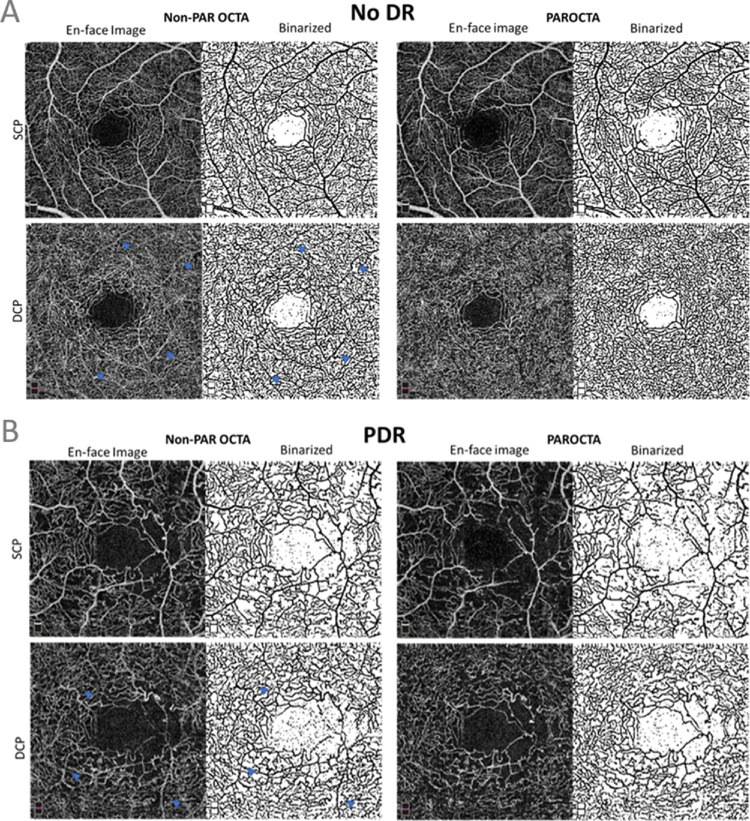
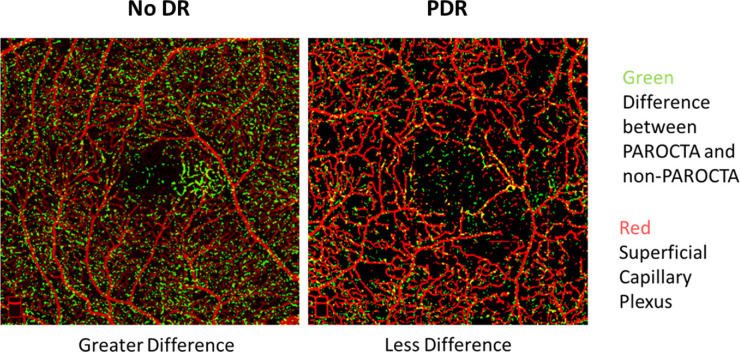
Purpose: The purpose of this study was to assess how projection artifact removal (PAR) alters optical coherence tomography angiography (OCTA) assessment of superficial capillary plexus (SCP) and deep capillary plexus (DCP) in eyes of patients with diabetes.
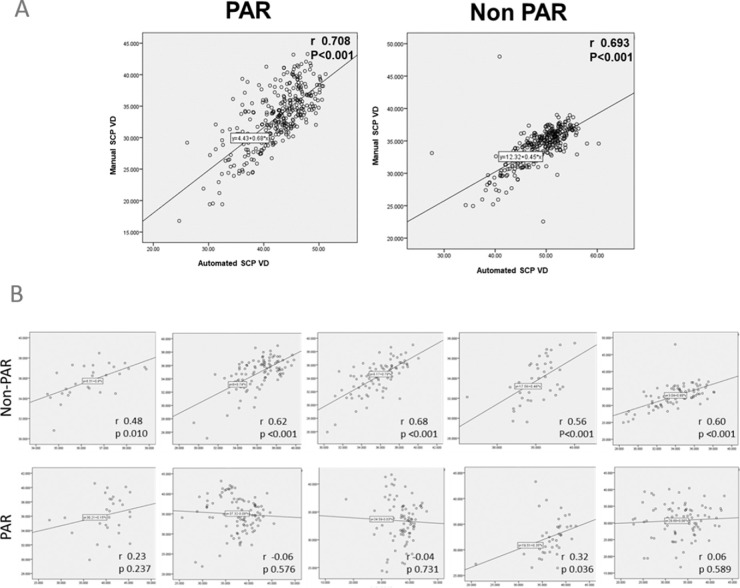
Methods: We acquired 3 × 3 mm scans with RTVue-XR Avanti (Optovue, Inc., Fremont, CA), which were analyzed with PAR software (PAROCTA) and without (non-PAROCTA). SCP, DCP, and full thickness retina vascular density (VD) and vessel linear density (VLD) were manually calculated using ImageJ (version 1.51). Adjusted flow index (AFI) was manually assessed for full thickness images.
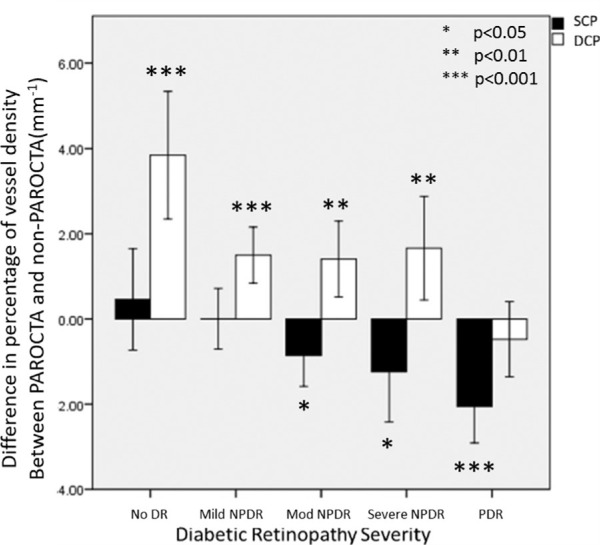
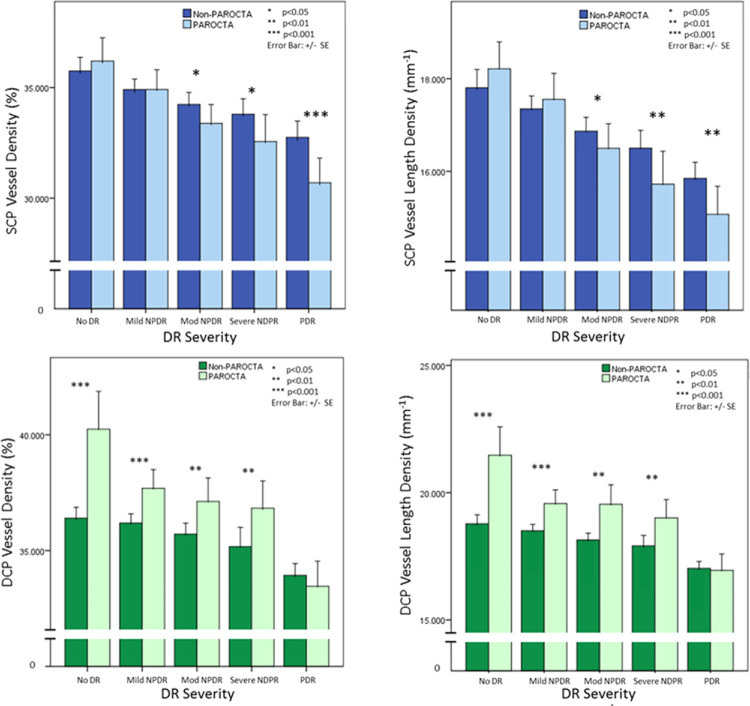
Results: Among 323 eyes of 194 patients (no diabetic retinopathy [DR]: 28 eyes; mild nonproliferative DR (NPDR): 96 eyes; moderate: 82 eyes; severe: 32 eyes; and proliferative DR [PDR]: 81 eyes), SCP VD and VLD were lower with PAROCTA than with non-PAROCTA only in eyes with moderate (VD: P = 0.017; VLD: P = 0.046), severe (P = 0.016; P = 0.009), and PDR (P < 0.001; P = 0.002). DCP VD and VLD were higher with PAROCTA as compared to non-PAROCTA only in eyes with no DR (VD and VLD: P < 0.001), mild (VD and VLD: P < 0.001), moderate (VD: P = 0.005; and VLD: P < 0.001), and severe (VD: P = 0.009; VLD: P < 0.001). Full thickness PAROCTA and non-PAROCTA VD and VLD differed only in eyes with no DR where PAROCTA estimates were higher (VD: P = 0.009; VLD: P = 0.02). PAROCTA AFI was lower than non-PAROCTA AFI for all DR severity levels (P < 0.001) except no DR.
Conclusions: Although differential effects of PAROCTA software are expected on SCP versus DCP measurements, these findings also suggest an interaction between PAROCTA and DR severity on assessment of VD. Conclusions from previous studies that have not corrected VD with PAR software should be carefully reviewed with regard to the role of specific vascular layers in DR.
Translational relevance: Previous OCTA studies that have not corrected VD with PAR software should be carefully reviewed with regard to the role of individual vascular layers in differing severity levels of DR.
Keywords: diabetic retinopathy imaging; optical coherence tomography angiography; retina.
Copyright 2020 The Authors.
Conflict of interest statement
Disclosure: M. Ashraf, None; K. Sampani, None; O. Abu-Qamar, None; J. Cavallerano, None; P.S. Silva, None; L.P. Aiello, None; J.K. Sun, Optovue (F)
Figures

References
-
- Dimitrova G, Chihara E, Takahashi H, Amano H, Okazaki K. Quantitative retinal optical coherence tomography angiography in patients with diabetes without diabetic retinopathy. Invest Ophthalmol Vis Sci. 2017; 58: 190–196. - PubMed
-
- Vujosevic S, Muraca A, Alkabes M, et al. .. Early microvascular and neural changes in patients with type 1 and type 2 diabetes mellitus without clinical signs of diabetic retinopathy. Retina. 2019; 39: 435–445. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
