

Glycemic control and risk factors for in-hospital mortality and vascular complications after coronary artery bypass grafting in patients with and without preexisting diabetes
- PMID: 32833247
- PMCID: PMC7891320
- DOI: 10.1111/1753-0407.13108
Glycemic control and risk factors for in-hospital mortality and vascular complications after coronary artery bypass grafting in patients with and without preexisting diabetes
Abstract
Background: The purpose of this study was to investigate risk factors of in-hospital mortality and vascular complications after coronary artery bypass grafting (CABG), particularly the effect of different glycemic control levels on outcomes in patients with and without previous evidence of diabetes.
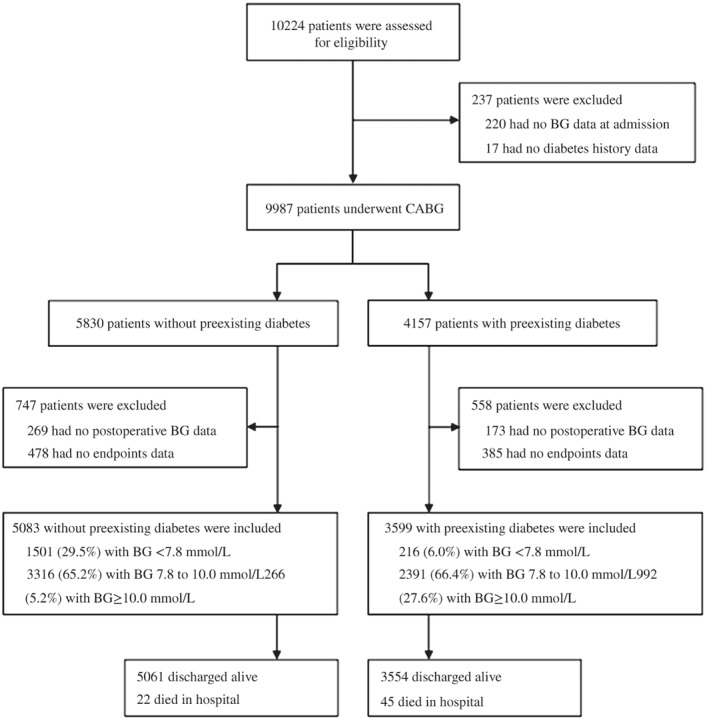
Methods: A total of 8682 patients with and without previous diabetes undergoing CABG were categorized into strict, moderate, and liberal glucose control groups according to their mean blood glucose control level <7.8 mmol/L, 7.8 to 10.0 mmol/L, and ≥10.0 mmoL/L after in-hospital CABG.
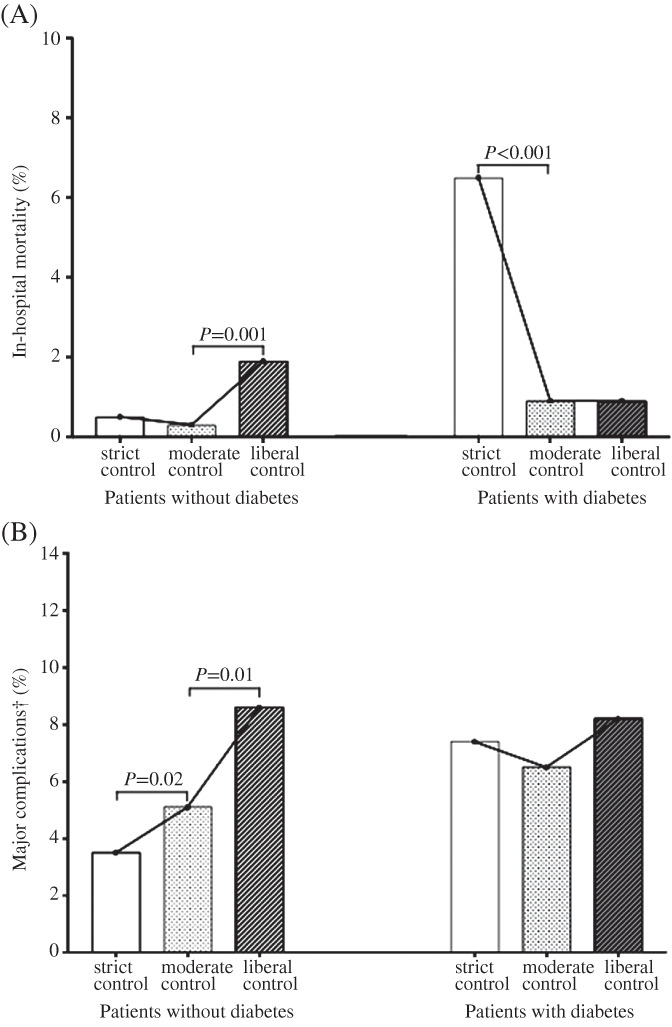
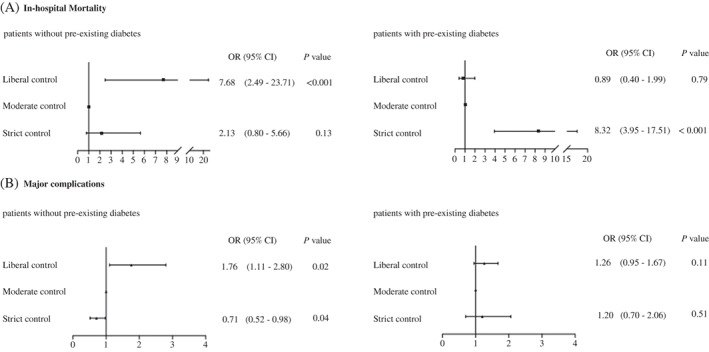
Results: The patients with previous diabetes had higher rates of in-hospital mortality (1.3% vs 0.4%, P < .001) and major complications (7.0% vs 4.8%, P < .001) than those without diabetes. Current diabetes was significantly associated with a higher risk of in-hospital mortality (odds ratio [OR] = 3.14, 95% confidence interval [CI] 1.87-5.27) and major complications (OR = 1.49, 95% CI 1.24-1.80), and smoking and higher low-density lipoprotein cholesterol (LDL-C) levels showed similar results. Among patients with previous diabetes, strict glucose control was significantly associated with an increased risk of in-hospital mortality (OR = 8.32, 95% CI 3.95-17.51) compared with moderate glucose control. Nevertheless, among non-previous diabetic patients with stress hyperglycemia, strict glucose control led to a lower risk of major complications (OR = 0.71, 95% CI 0.52-0.98).
Conclusions: Diabetes status, smoking, and LDL-C levels were modifiable risk factors of both in-hospital mortality and major complications after CABG. Strict glucose control was associated with an increased risk of in-hospital mortality among patients with diabetes, whereas it reduced the risk of major complications among non-previous diabetic patients.
目的: 探讨冠状动脉旁路移植术患者院内死亡和血管并发症的影响因素, 重点分析不同血糖控制水平对有, 无糖尿病史患者术后并发症的影响。 方法: 8682名接受冠状动脉旁路移植术治疗患者依术后平均血糖控制水平分为严格, 中度和宽松血糖控制三个组。各组平均血糖值依次为<7.8mmol/L, 7.8-10.0mmol/L和≥10.0mmoL/L。 结果: 有糖尿病史的患者院内死亡率及术后主要并发症明显高于无糖尿病史患者(院内死亡率:1.3% vs 0.4%, P <0 .001; 主要并发症:7.0% vs 4.8%, P <0 .001)。糖尿病状态显著增加院内死亡风险(OR:3.14, 95%CI:1.87-5.27)和主要并发症风险(OR = 1.49, 95%CI 1.24-1.80); 吸烟及低密度脂蛋白胆固醇升高亦增加死亡和主要并发症风险。在有糖尿病史患者中, 与中度血糖控制组相比, 严格血糖控制组院内死亡风险明显增加(OR:8.32, 95% CI:3.95-17.51)。与之相反, 在无糖尿病史患者中, 严格血糖控制组的主要并发症风险却明显减少(OR:0.71,95% CI:0.52-0.98)。 结论: 糖尿病, 吸烟和低密度脂蛋白胆固醇升高是冠状动脉旁路移植术后院内死亡和主要并发症的三个可变危险因素。严格血糖控制增加糖尿病手术患者院内死亡风险, 但却可以减少非糖尿病患者术后主要并发症风险。.
Keywords: complications; coronary artery bypass grafting; diabetes; mortality; risk factor; 冠状动脉旁路移植术; 危险因素; 并发症; 死亡率; 糖尿病.
© 2020 The Authors. Journal of Diabetes published by Ruijin Hospital, Shanghai JiaoTong University School of Medicine and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Superiority of moderate control of hyperglycemia to tight control in patients undergoing coronary artery bypass grafting.J Thorac Cardiovasc Surg. 2011 Feb;141(2):543-51. doi: 10.1016/j.jtcvs.2010.10.005. Epub 2010 Dec 15. J Thorac Cardiovasc Surg. 2011. PMID: 21163498 Free PMC article.
-
Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting.J Thorac Cardiovasc Surg. 2003 May;125(5):1007-21. doi: 10.1067/mtc.2003.181. J Thorac Cardiovasc Surg. 2003. PMID: 12771873 Clinical Trial.
-
Effects of aggressive versus moderate glycemic control on clinical outcomes in diabetic coronary artery bypass graft patients.Ann Surg. 2011 Sep;254(3):458-63; discussion 463-4. doi: 10.1097/SLA.0b013e31822c5d78. Ann Surg. 2011. PMID: 21865944 Clinical Trial.
-
Prior Percutaneous Coronary Intervention and Mortality in Patients Undergoing Surgical Myocardial Revascularization: Results From the E-CABG (European Multicenter Study on Coronary Artery Bypass Grafting) With a Systematic Review and Meta-Analysis.Circ Cardiovasc Interv. 2018 Feb;11(2):e005650. doi: 10.1161/CIRCINTERVENTIONS.117.005650. Circ Cardiovasc Interv. 2018. PMID: 29440275
-
Stroke Rates Following Surgical Versus Percutaneous Coronary Revascularization.J Am Coll Cardiol. 2018 Jul 24;72(4):386-398. doi: 10.1016/j.jacc.2018.04.071. J Am Coll Cardiol. 2018. PMID: 30025574
Cited by
-
Perioperative glycemic control in patients undergoing cardiac surgery.Kardiochir Torakochirurgia Pol. 2025 Mar;22(1):44-52. doi: 10.5114/kitp.2025.148548. Epub 2025 Mar 17. Kardiochir Torakochirurgia Pol. 2025. PMID: 40290708 Free PMC article. Review.
-
Effect of glycemic control and glucose fluctuation on in-hospital adverse outcomes after on-pump coronary artery bypass grafting in patients with diabetes: a retrospective study.Diabetol Metab Syndr. 2023 Feb 14;15(1):20. doi: 10.1186/s13098-023-00984-4. Diabetol Metab Syndr. 2023. PMID: 36788548 Free PMC article.
-
The efficacy of minimally invasive coronary artery bypass grafting (mics cabg) for patients with coronary artery diseases and diabetes: a single center retrospective study.J Cardiothorac Surg. 2024 Apr 18;19(1):244. doi: 10.1186/s13019-024-02717-8. J Cardiothorac Surg. 2024. PMID: 38632609 Free PMC article.
-
Active Detection of Glucose Metabolism Disorders Prior to Coronary Artery Bypass Grafting: Associations with In-Hospital Postoperative Complications.J Clin Med. 2025 Apr 30;14(9):3123. doi: 10.3390/jcm14093123. J Clin Med. 2025. PMID: 40364157 Free PMC article.
-
7-year outcomes in diabetic patients after coronary artery bypass graft in a developing country.BMC Cardiovasc Disord. 2023 May 12;23(1):248. doi: 10.1186/s12872-023-03279-8. BMC Cardiovasc Disord. 2023. PMID: 37173658 Free PMC article.
References
-
- Weisel RD, Nussmeier N, Newman MF, et al. Predictors of contemporary coronary artery bypass grafting outcomes. J Thorac Cardiovasc Surg. 2014;148(6):2720‐2726. - PubMed
-
- Yoo JS, Kim JB, Jung SH, Choo SJ, Chung CH, Lee JW. Coronary artery bypass grafting in patients with left ventricular dysfunction: predictors of long‐term survival and impact of surgical strategies. Int J Cardiol. 2013;168:5316‐5322. - PubMed
-
- Holly TA, Bonow RO, Arnold JM, et al. Myocardial viability and impact of surgical ventricular reconstruction on outcomes of patients with severe left ventricular dysfunction undergoing coronary artery bypass surgery: results of the surgical treatment for ischemic heart failure trial. J Thorac Cardiovasc Surg. 2014;148:2677‐2684. - PMC - PubMed
