

Prism adaptation treatment for upper-limb complex regional pain syndrome: a double-blind randomized controlled trial
- PMID: 32833791
- PMCID: PMC7808368
- DOI: 10.1097/j.pain.0000000000002053
Prism adaptation treatment for upper-limb complex regional pain syndrome: a double-blind randomized controlled trial
Abstract
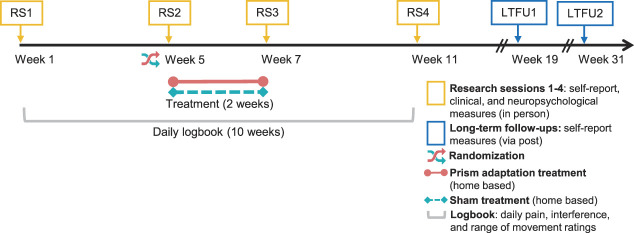
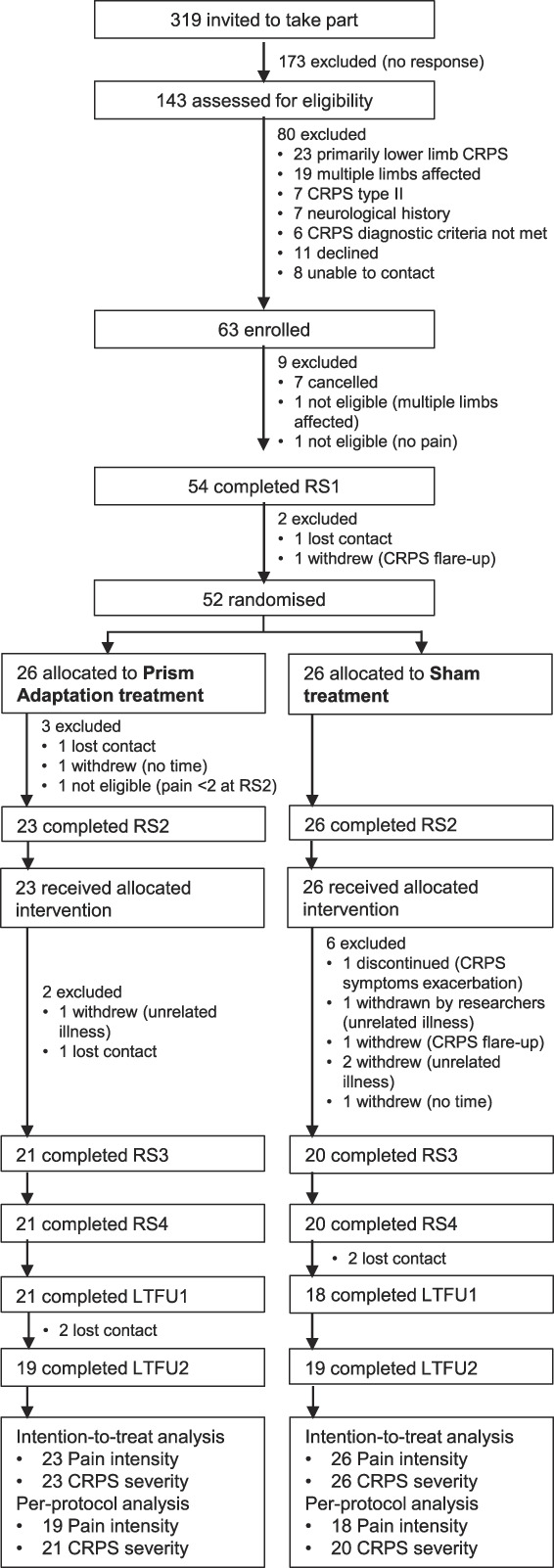
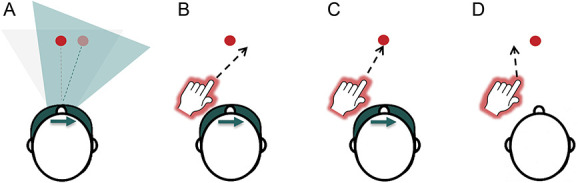
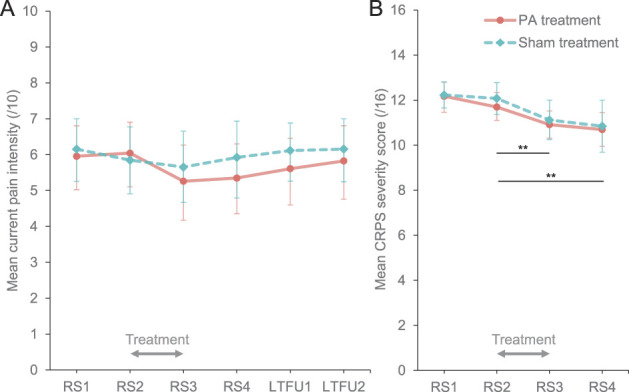
Initial evidence suggested that people with complex regional pain syndrome (CRPS) have reduced attention to the affected side of their body and the surrounding space, which might be related to pain and other clinical symptoms. Three previous unblinded, uncontrolled studies showed pain relief after treatment with prism adaptation, an intervention that has been used to counter lateralised attention bias in brain-lesioned patients. To provide a robust test of its effectiveness for CRPS, we conducted a double-blind randomized controlled trial of prism adaptation for unilateral upper-limb CRPS-I. Forty-nine eligible adults with CRPS were randomized to undergo 2 weeks of twice-daily home-based prism adaptation treatment (n = 23) or sham treatment (n = 26). Outcomes were assessed in person 4 weeks before and immediately before treatment, and immediately after and 4 weeks after treatment. Long-term postal follow-ups were conducted 3 and 6 months after treatment. We examined the effects of prism adaptation vs sham treatment on current pain intensity and the CRPS symptom severity score (primary outcomes), as well as sensory, motor, and autonomic functions, self-reported psychological functioning, and experimentally tested neuropsychological functions (secondary outcomes). We found no evidence that primary or secondary outcomes differed between the prism adaptation and sham treatment groups when tested at either time point after treatment. Overall, CRPS severity significantly decreased over time for both groups, but we found no benefits of prism adaptation beyond sham treatment. Our findings do not support the efficacy of prism adaptation treatment for relieving upper-limb CRPS-I. This trial was prospectively registered (ISRCTN46828292).
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the International Association for the Study of Pain.
Conflict of interest statement
M. Halicka and A.D. Vittersø were supported by studentships from the University of Bath and the GW4 BioMed Medical Research Council Doctoral Training Partnership (ref. 1793344), respectively. H. McCullough and A. Goebel have received support from the Pain Relief Foundation, Liverpool. A. Goebel, L. Heelas, and J.H. Bultitude are committee members of the CRPS-UK Research Network. L. Heelas is a committee member of the Physiotherapy Pain Association and the British Pain Society. The authors have no other competing interests to declare.
Oral presentations of the preliminary results were delivered at the UK Sensorimotor Conference in London, UK (2019), and the Pain Research Meeting in Brussels, Belgium (2019).
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- Bean DJ, Johnson MH, Kydd RR. The outcome of complex regional pain syndrome type 1: a systematic review. J Pain 2014;15:677–90. - PubMed
-
- Beerthuizen A, Stronks DL, van't Spijker A, Yaksh A, Hanraets BM, Klein J, Huygen FJPM. Demographic and medical parameters in the development of complex regional pain syndrome type 1 (CRPS1): prospective study on 596 patients with a fracture. PAIN 2012;153:1187–92. - PubMed
-
- Berberovic N, Pisella L, Morris AP, Mattingley JB. Prismatic adaptation reduces biased temporal order judgements in spatial neglect. Neuroreport 2004;15:1199–204. - PubMed
-
- Bingel U, Wanigasekera V, Wiech K, Mhuircheartaigh RN, Lee MC, Ploner M, Tracey I. The effect of treatment expectation on drug efficacy: imaging the analgesic benefit of the opioid remifentanil. Sci Transl Med 2011;3:70ra14. - PubMed
-
- Birklein F, Schlereth T. Complex regional pain syndrome—significant progress in understanding. PAIN 2015;156:S94–S103. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
