

GM-CSF blockade with mavrilimumab in severe COVID-19 pneumonia and systemic hyperinflammation: a single-centre, prospective cohort study
- PMID: 32835256
- PMCID: PMC7430344
- DOI: 10.1016/S2665-9913(20)30170-3
GM-CSF blockade with mavrilimumab in severe COVID-19 pneumonia and systemic hyperinflammation: a single-centre, prospective cohort study
Abstract
Background: Mortality in patients with COVID-19 pneumonia and systemic hyperinflammation is high. We aimed to examine whether mavrilimumab, an anti-granulocyte-macrophage colony-stimulating factor receptor-α monoclonal antibody, added to standard management, improves clinical outcomes in patients with COVID-19 pneumonia and systemic hyperinflammation.
Methods: This single-centre prospective cohort study included patients aged 18 years or older who were admitted to San Raffaele Hospital (Milan, Italy) with severe COVID-19 pneumonia, hypoxia, and systemic hyperinflammation. Patients received a single intravenous dose (6 mg/kg) of mavrilimumab added to standard care given by the hospital at the time. The control group consisted of contemporaneous patients with similar baseline characteristics who received standard care at the same hospital. The main outcome was time to clinical improvement (defined as improvement of two or more points on the seven-point ordinal scale of clinical status). Other outcomes included proportion of patients achieving clinical improvement, survival, mechanical ventilation-free survival, and time to fever resolution. Adverse events were monitored daily.
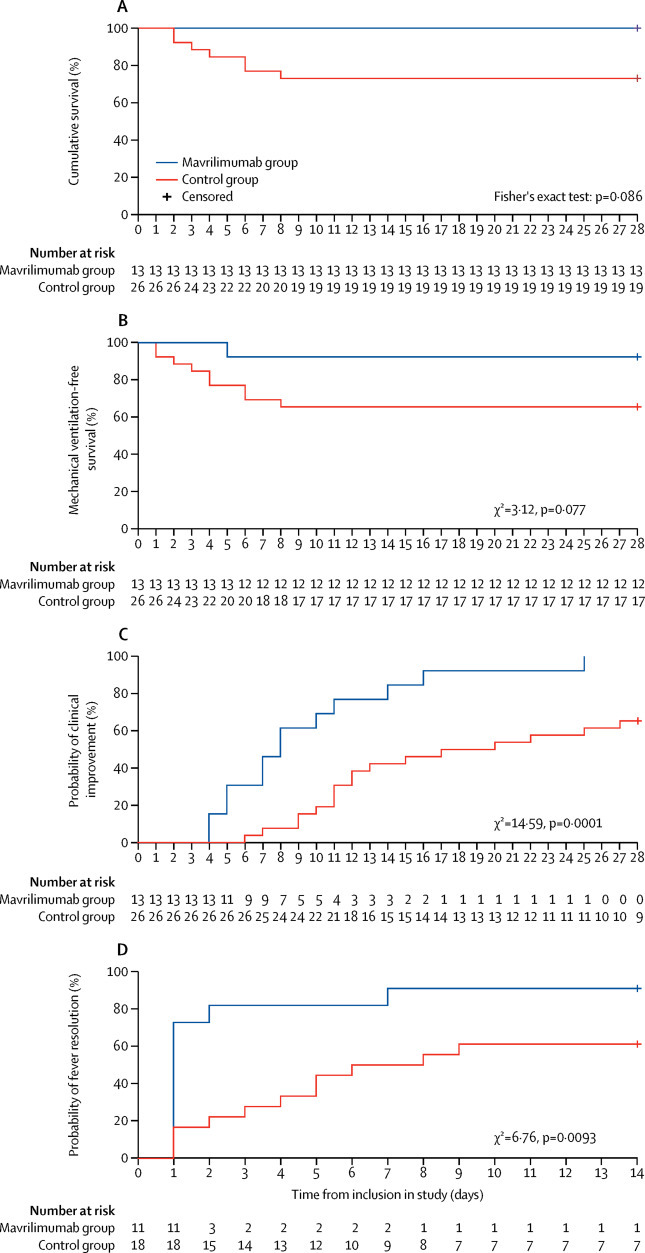
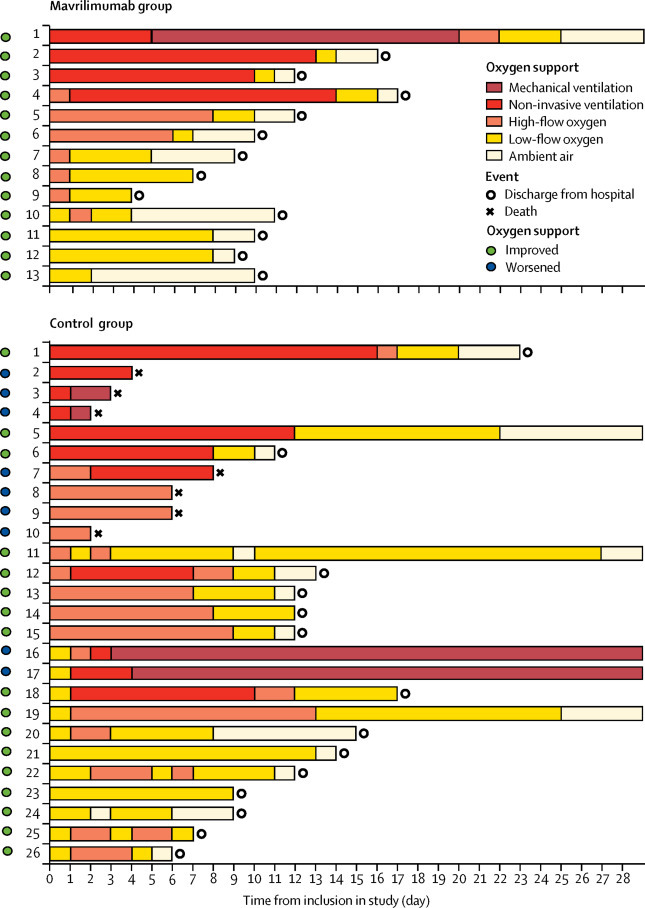
Findings: Between March 17 and April 15, 2020, 13 non-mechanically ventilated patients (median age 57 years [IQR 52-58], 12 [92%] men) received mavrilimumab and 26 patients (median age 60 [IQR 53-67], 17 [65%] men) in the control group received standard care. During the 28-day follow-up, no patients in the mavrilimumab group died, and seven (27%) patients in the control group died (p=0·086). At day 28, all patients in the mavrilimumab group and 17 (65%) patients in the control group showed clinical improvement (p=0·030), with earlier improvement in the mavrilimumab than in the control group (mean time to improvement 8 days [IQR 5 to 11] vs 19 days [11 to >28], p=0·0001). By day 28, one (8%) patient in the mavrilimumab group progressed to mechanical ventilation compared with nine (35%) patients in the control group who progressed to mechanical ventilation or died (p=0·14). By day 14, fever resolved in ten (91%) of 11 febrile patients in the mavrilimumab group, compared with 11 (61%) of 18 febrile patients in the control group (p=0·18); fever resolution was faster in mavrilimumab recipients versus controls (median time to resolution 1 day [IQR 1 to 2] vs 7 days [3 to >14], p=0·0093). Mavrilimumab was well tolerated, with no infusion reactions. Three (12%) patients in the control group developed infectious complications.
Interpretation: Mavrilimumab treatment was associated with improved clinical outcomes compared with standard care in non-mechanically ventilated patients with severe COVID-19 pneumonia and systemic hyperinflammation. Treatment was well tolerated. Confirmation of efficacy requires controlled testing.
Funding: IRCCS San Raffaele Scientific Institute.
© 2020 Elsevier Ltd. All rights reserved.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
