

Rapid Generation of Neutralizing Antibody Responses in COVID-19 Patients
- PMID: 32835303
- PMCID: PMC7276302
- DOI: 10.1016/j.xcrm.2020.100040
Rapid Generation of Neutralizing Antibody Responses in COVID-19 Patients
Abstract
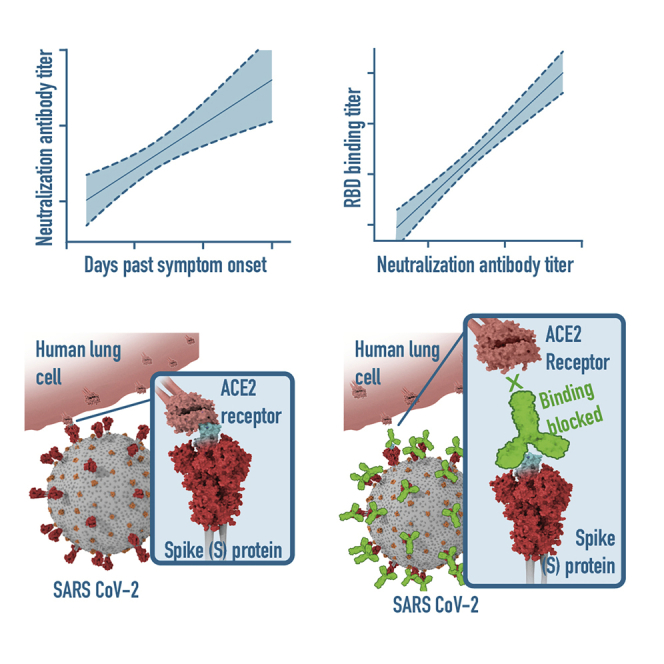
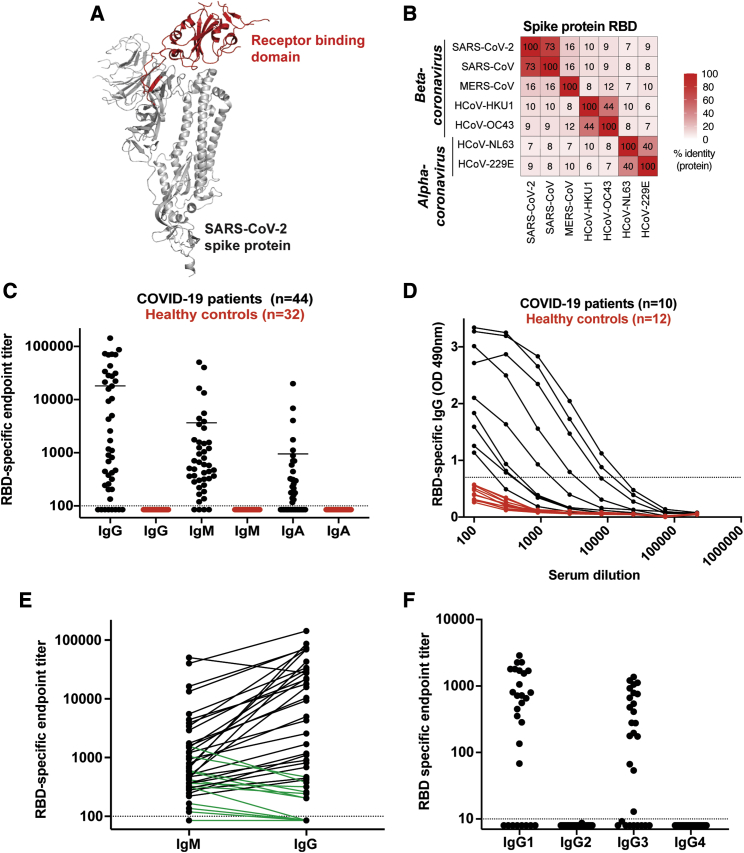
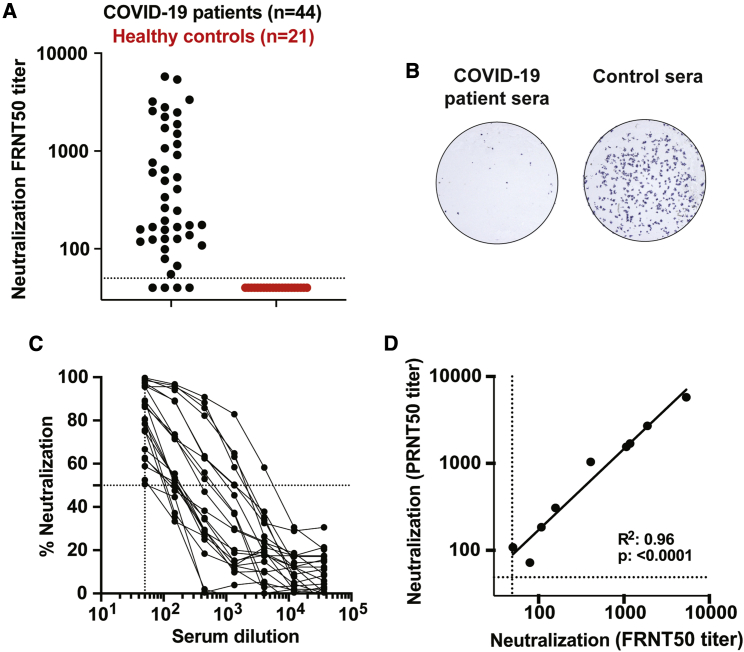
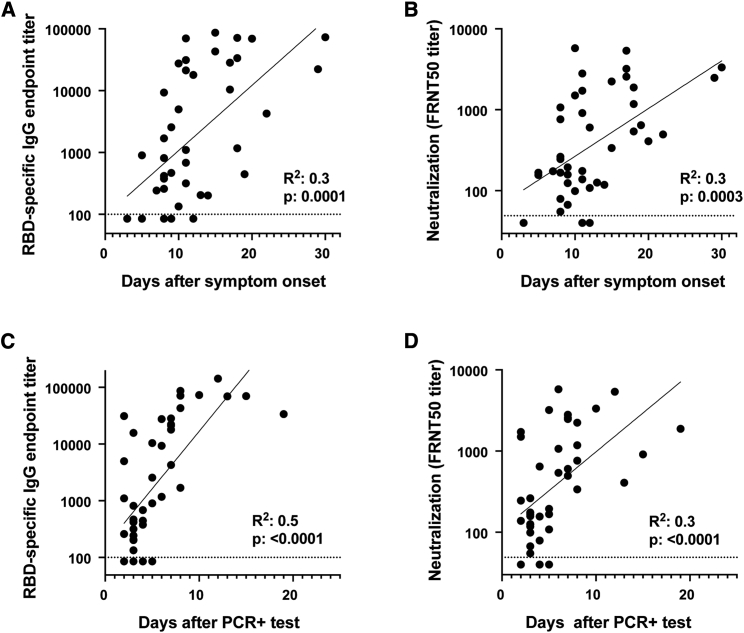
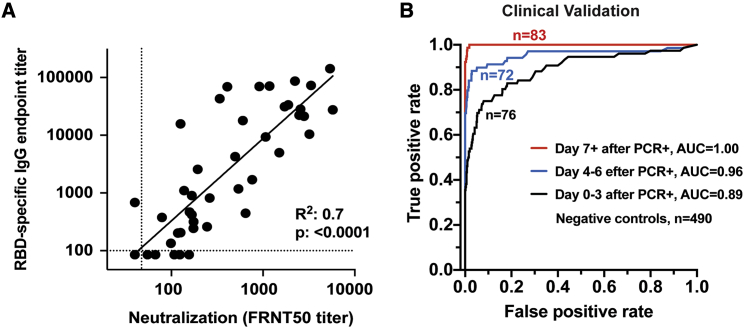
SARS-CoV-2, the virus responsible for COVID-19, is causing a devastating worldwide pandemic, and there is a pressing need to understand the development, specificity, and neutralizing potency of humoral immune responses during acute infection. We report a cross-sectional study of antibody responses to the receptor-binding domain (RBD) of the spike protein and virus neutralization activity in a cohort of 44 hospitalized COVID-19 patients. RBD-specific IgG responses are detectable in all patients 6 days after PCR confirmation. Isotype switching to IgG occurs rapidly, primarily to IgG1 and IgG3. Using a clinical SARS-CoV-2 isolate, neutralizing antibody titers are detectable in all patients by 6 days after PCR confirmation and correlate with RBD-specific binding IgG titers. The RBD-specific binding data were further validated in a clinical setting with 231 PCR-confirmed COVID-19 patient samples. These findings have implications for understanding protective immunity against SARS-CoV-2, therapeutic use of immune plasma, and development of much-needed vaccines.
Keywords: COVID-19; SARS-CoV-2; coronavirus; humoral immune response; neutralizing antibody; protective immunity; receptor-binding protein; serology test; spike protein.
© 2020 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
Rapid generation of neutralizing antibody responses in COVID-19 patients.medRxiv [Preprint]. 2020 May 8:2020.05.03.20084442. doi: 10.1101/2020.05.03.20084442. medRxiv. 2020. Update in: Cell Rep Med. 2020 Jun 23;1(3):100040. doi: 10.1016/j.xcrm.2020.100040. PMID: 32511565 Free PMC article. Updated. Preprint.
References
Grants and funding
- R38 AI140299/AI/NIAID NIH HHS/United States
- T32 GM008169/GM/NIGMS NIH HHS/United States
- R00 AG049092/AG/NIA NIH HHS/United States
- U19 AI057266/AI/NIAID NIH HHS/United States
- T32 AI074492/AI/NIAID NIH HHS/United States
- UM1 AI148684/AI/NIAID NIH HHS/United States
- R24 AI120942/AI/NIAID NIH HHS/United States
- K99 AI153736/AI/NIAID NIH HHS/United States
- U01 AI151801/AI/NIAID NIH HHS/United States
- R01 AI137127/AI/NIAID NIH HHS/United States
- U19 AI090023/AI/NIAID NIH HHS/United States
- P51 OD011132/OD/NIH HHS/United States
- UM1 AI148576/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
