

SARS-CoV-2 infection in pregnancy: A systematic review and meta-analysis of clinical features and pregnancy outcomes
- PMID: 32838230
- PMCID: PMC7334039
- DOI: 10.1016/j.eclinm.2020.100446
SARS-CoV-2 infection in pregnancy: A systematic review and meta-analysis of clinical features and pregnancy outcomes
Abstract
Background: Perform a systematic review and meta-analysis of SARS-CoV-2 infection and pregnancy.
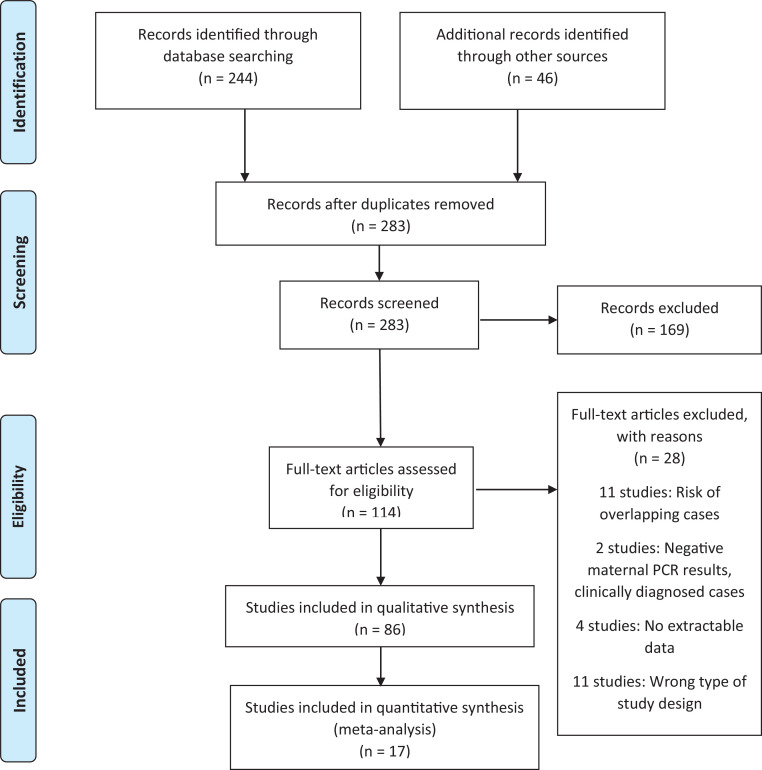
Methods: Databases (Medline, Embase, Clinicaltrials.gov, Cochrane Library) were searched electronically on 6th April and updated regularly until 8th June 2020. Reports of pregnant women with reverse transcription PCR (RT-PCR) confirmed COVID-19 were included. Meta-analytical proportion summaries and meta-regression analyses for key clinical outcomes are provided.
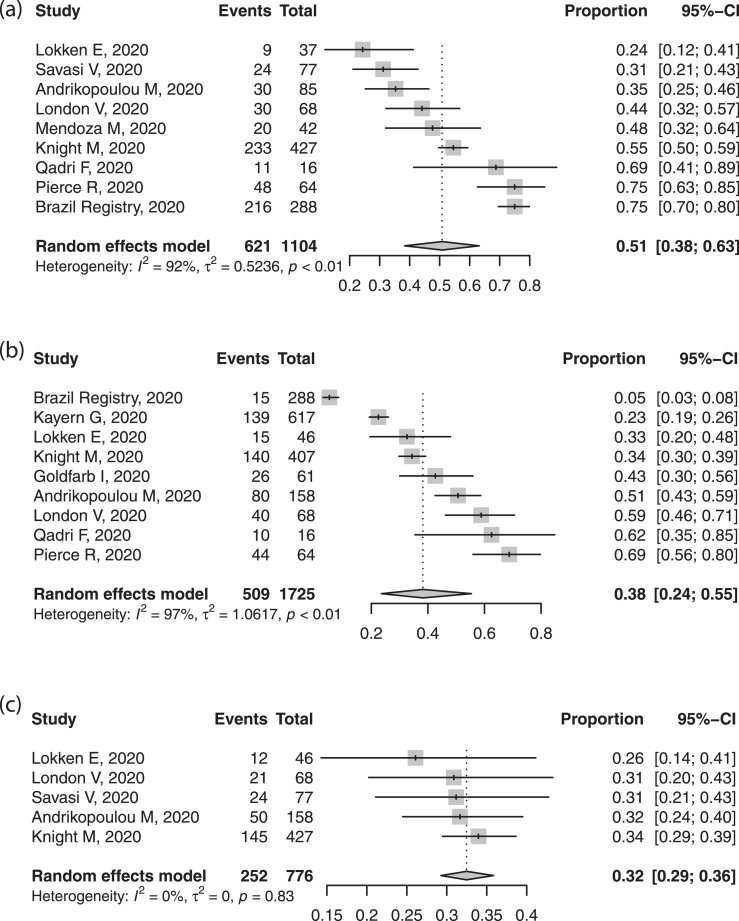
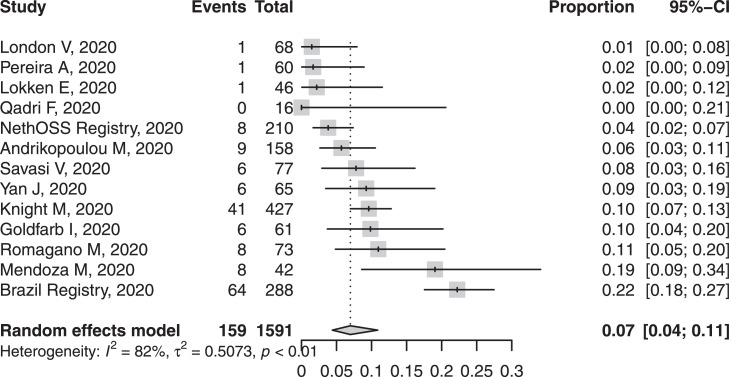
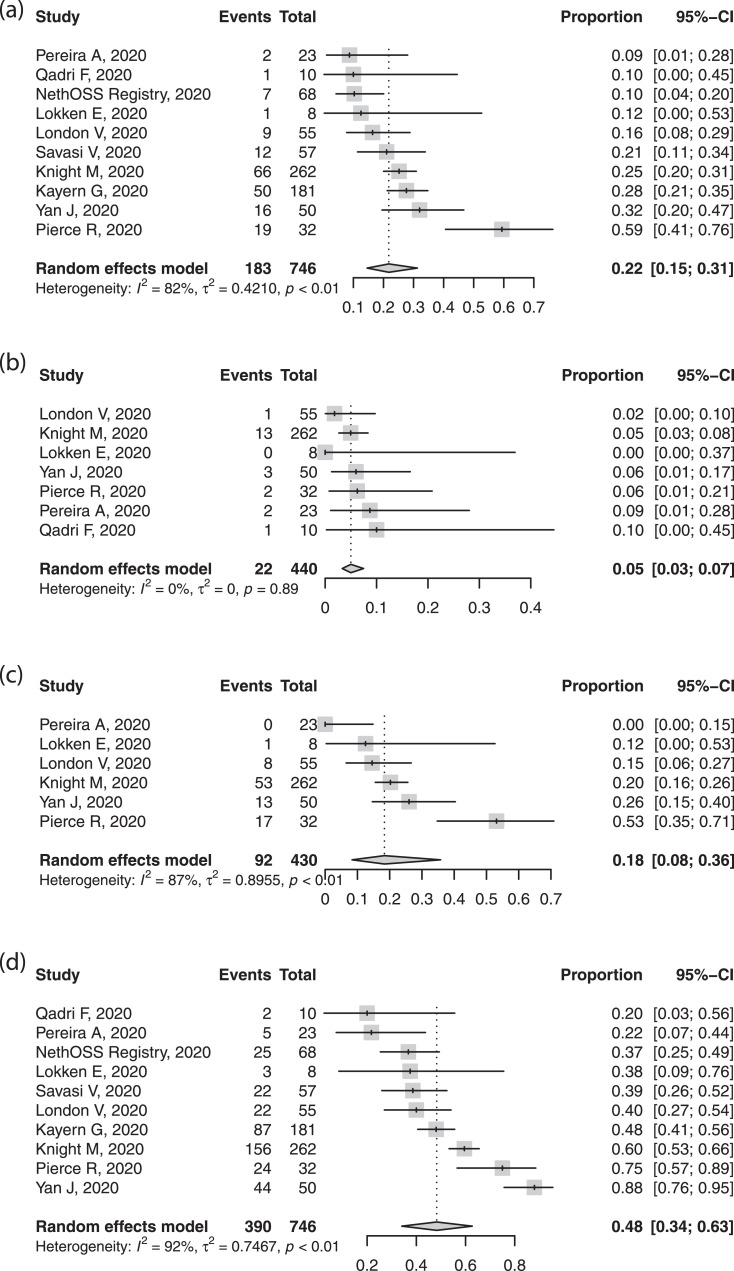
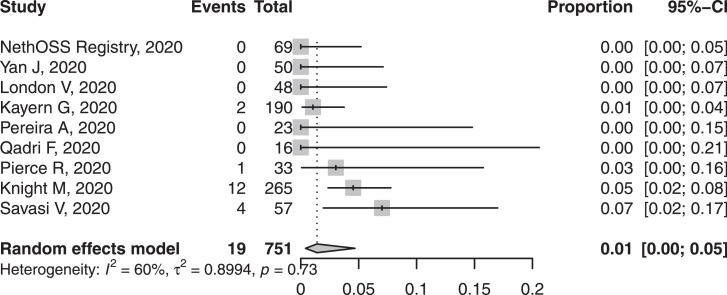
Findings: 86 studies were included, 17 studies (2567 pregnancies) in the quantitative synthesis; other small case series and case reports were used to extract rarely-reported events and outcome. Most women (73.9%) were in the third trimester; 52.4% have delivered, half by caesarean section (48.3%). The proportion of Black, Asian or minority ethnic group membership (50.8%); obesity (38.2%), and chronic co-morbidities (32.5%) were high. The most commonly reported clinical symptoms were fever (63.3%), cough (71.4%) and dyspnoea (34.4%). The commonest laboratory abnormalities were raised CRP or procalcitonin (54.0%), lymphopenia (34.2%) and elevated transaminases (16.0%). Preterm birth before 37 weeks' gestation was common (21.8%), usually medically-indicated (18.4%). Maternal intensive care unit admission was required in 7.0%, with intubation in 3.4%. Maternal mortality was uncommon (~1%). Maternal intensive care admission was higher in cohorts with higher rates of co-morbidities (beta=0.007, p<0.05) and maternal age over 35 years (beta=0.007, p<0.01). Maternal mortality was higher in cohorts with higher rates of antiviral drug use (beta=0.03, p<0.001), likely due to residual confounding. Neonatal nasopharyngeal swab RT-PCR was positive in 1.4%.
Interpretation: The risk of iatrogenic preterm birth and caesarean delivery was increased. The available evidence is reassuring, suggesting that maternal morbidity is similar to that of women of reproductive age. Vertical transmission of the virus probably occurs, albeit in a small proportion of cases.
Funding: N/A.
© 2020 The Author(s).
Conflict of interest statement
Dr. Morris is the President and Trustee of the Royal College of Obstetricians and Gynaecologists. He is a Trustee of the British Menopause Society and the Chairman of the Baby Lifeline Multiprofessional Advisory Panel.
Figures
References
-
- World Health Organization. WHO Timeline - COVID-19. 2020. [online] Who.int. Available at: <https://www.who.int/news-room/detail/08-04-2020-who-timeline—covid-19>... 10 April 2020].
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
