

Community-based cluster randomized controlled trial: empowering households to identify and provide appropriate care for low-birthweight newborns in Nepal
- PMID: 32838783
- PMCID: PMC7446145
- DOI: 10.1186/s12889-020-09317-w
Community-based cluster randomized controlled trial: empowering households to identify and provide appropriate care for low-birthweight newborns in Nepal
Abstract
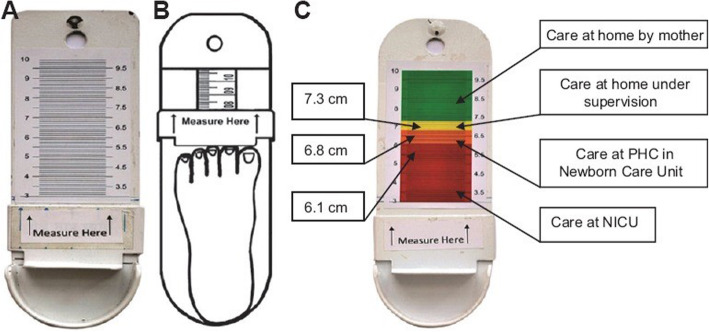
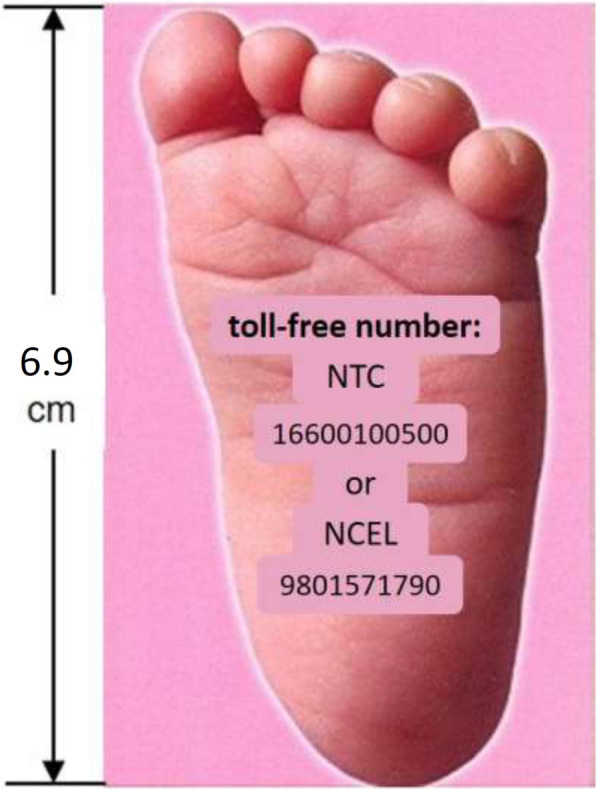
Background: Most newborn deaths occur among those of low birthweight (LBWt), due to prematurity &/or impaired fetal growth. Simple practices can substantially mitigate this risk. In low-income country settings where many births occur at home, strategies are needed that empower mothers to determine if their babies are at higher risk and, if so, to take measures to reduce risk. Earlier studies suggest that foot-length may be a good proxy for birthweight. An earlier Nepal study found a 6.9 cm cut-off performed relatively well, differentiating normal from low birthweight.
Methods: Community-based, cluster-randomized controlled trial.
Objective: to determine whether family-administered screening, associated with targeted messages improves care practices known to mitigate LBWt-associated risks.
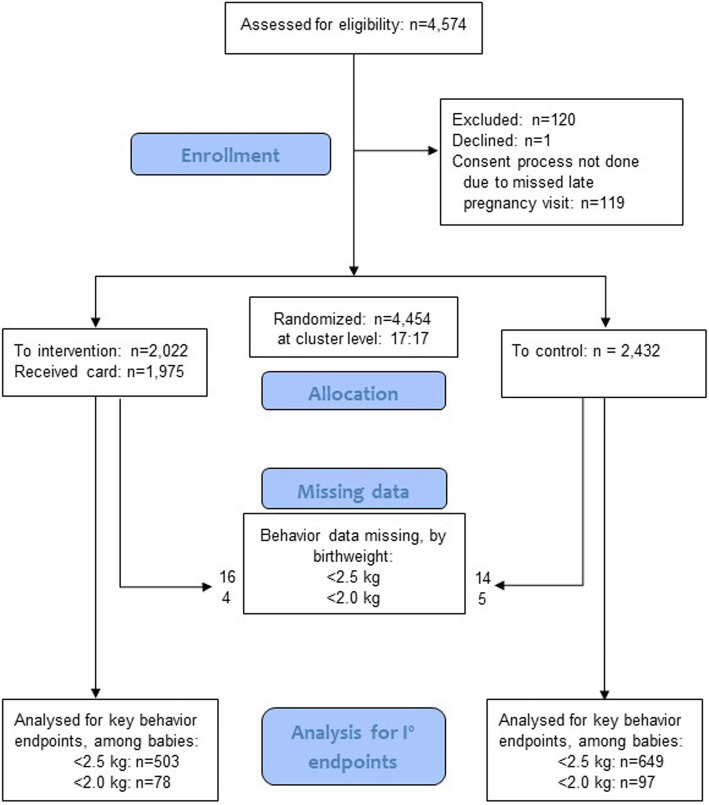
Participants: women participating in a parent trial in rural Nepal, recruited late in pregnancy. Women were given a 6.9 cm card to assess whether the baby's foot is small; if so, to call a number on the card for advice. Follow-up visits were made over the 2 weeks following the birth, assessing for 2 behavioral outcomes: reported skin-to-skin thermal care, and care-seeking outside the home; assessed restricting to low birthweight (using 2 cutoffs: 2500 g and 2000 g). Randomization: 17 clusters intervention, 17 control. The study also documented performance along the presumed causal chain from intervention through behavioral impact.
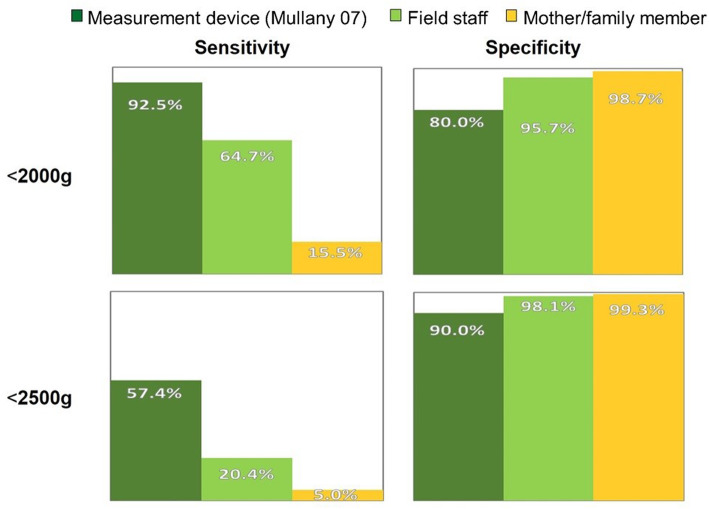
Results: 2022 intervention, 2432 control. Intervention arm: 519 had birthweight < 2500 g (vs. 663 among controls), of which 503 were available for analysis (vs. 649 among controls). No significant difference found on care-seeking; for those < 2500 g RR 1.13 (95%CI: 0.97-1.131). A higher proportion of those in the intervention arm reported skin-to-skin thermal care than among controls; for those < 2500 g RR 2.50 (95%CI: 2.01-3.1). However, process measures suggest this apparent effect cannot be attributed to the intervention; the card performed poorly as a proxy for LBWt, misclassifying 84.5% of those < 2000 as normal weight.
Conclusions: Although the trial found an apparent effect on one of the behavioral outcomes, this cannot be attributed to the intervention; most likely it was a result of pure chance. Other approaches are needed for identifying small, at-risk babies in such settings, and targeting them for appropriate care messaging.
Trial registration: ClinicalTrials.gov NCT02802332 , registered 6/16/2016.
Keywords: Anthropometry; Behavior change; Care-seeking; Home childbirth; Low birth-weight; Low- and middle-income countries; Sensitivity and specificity; Thermal care.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
