

A population-based phenome-wide association study of cardiac and aortic structure and function
- PMID: 32839619
- PMCID: PMC7613250
- DOI: 10.1038/s41591-020-1009-y
A population-based phenome-wide association study of cardiac and aortic structure and function
Abstract
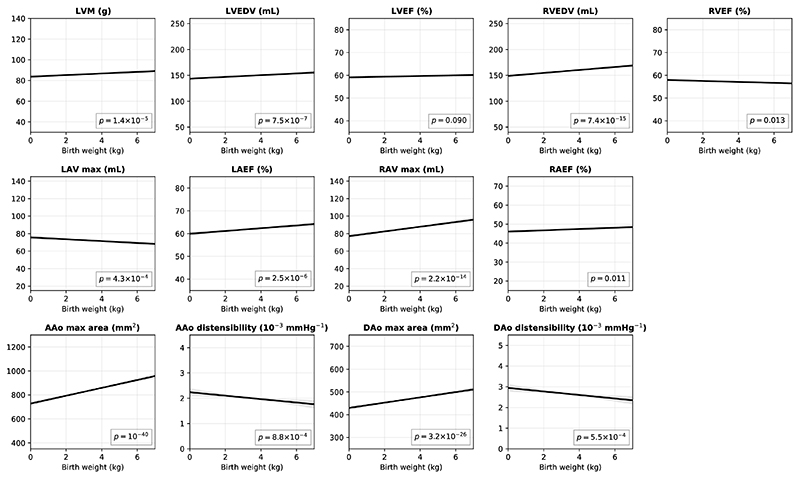
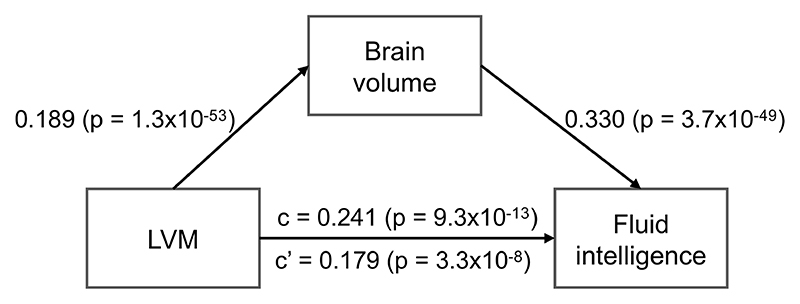
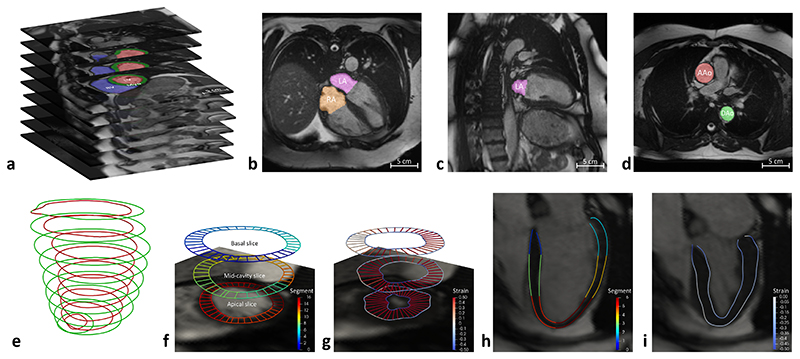
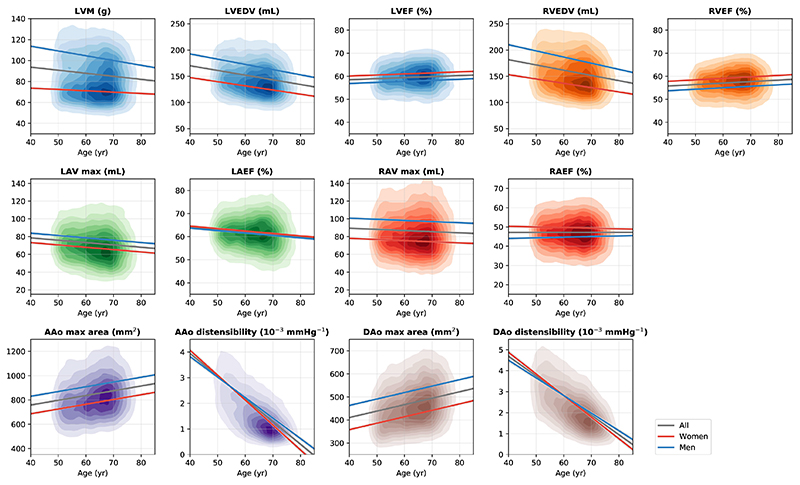
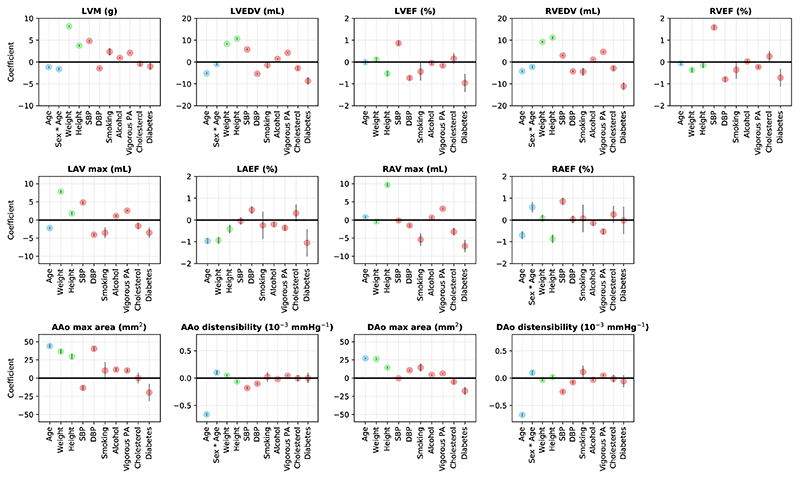
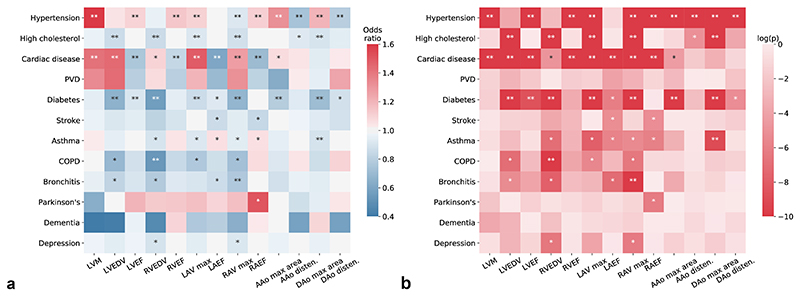
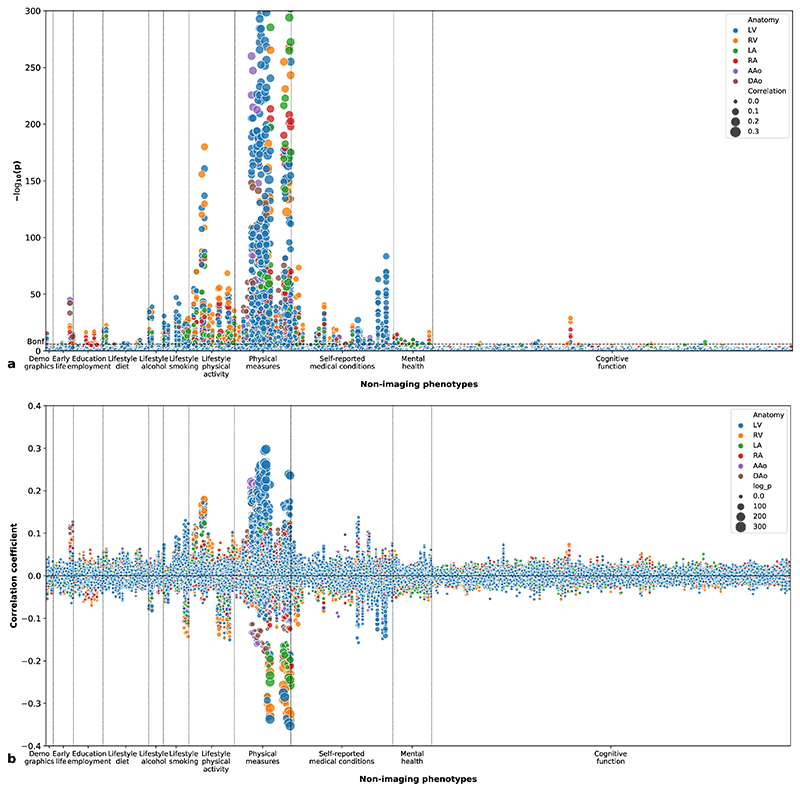
Differences in cardiac and aortic structure and function are associated with cardiovascular diseases and a wide range of other types of disease. Here we analyzed cardiovascular magnetic resonance images from a population-based study, the UK Biobank, using an automated machine-learning-based analysis pipeline. We report a comprehensive range of structural and functional phenotypes for the heart and aorta across 26,893 participants, and explore how these phenotypes vary according to sex, age and major cardiovascular risk factors. We extended this analysis with a phenome-wide association study, in which we tested for correlations of a wide range of non-imaging phenotypes of the participants with imaging phenotypes. We further explored the associations of imaging phenotypes with early-life factors, mental health and cognitive function using both observational analysis and Mendelian randomization. Our study illustrates how population-based cardiac and aortic imaging phenotypes can be used to better define cardiovascular disease risks as well as heart-brain health interactions, highlighting new opportunities for studying disease mechanisms and developing image-based biomarkers.
Conflict of interest statement
S.E.P. acknowledges consultancy fees from Circle Cardiovascular Imaging Inc., Calgary, Alberta, Canada. D.R. acknowledges consultancy fees from Circle Cardiovascular Imaging Inc., Calgary, Alberta, Canada, Heartflow, Redwood City, CA, USA and IXICO PLC, London, UK. P.M.M. acknowledges consultancy fees from Roche, Adelphi Communications, Celgene and Biogen. He has received honoraria or speakers’ honoraria from Novartis, Biogen and Roche and has received research or educational funds from Biogen, Novartis, GlaxoSmithKline and Nodthera. He is a member of the Scientific Advisory Board to the Board of Ipsen Pharmaceuticals. The remaining authors declare no competing interests.
Figures
References
-
- Ponikowski P, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur J Hear Fail. 2016;18:891–975. - PubMed
-
- Erbel R, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases. Eur Hear J. 2014;35:2873–2926. - PubMed
-
- Watz H, et al. Decreasing cardiac chamber sizes and associated heart dysfunction in COPD. Chest. 2010;138:32–38. - PubMed
-
- Alonso-Gonzalez R, et al. Abnormal lung function in adults with congenital heart disease: Prevalence, relation to cardiac anatomy, and association with survival. Circulation. 2013;127:882–890. - PubMed
-
- Gansevoort RT, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. The Lancet. 2013;382:339–352. - PubMed
Publication types
MeSH terms
Grants and funding
- FS/15/81/31817/BHF_/British Heart Foundation/United Kingdom
- RE/18/4/34215/BHF_/British Heart Foundation/United Kingdom
- MC-A651-53301/MRC_/Medical Research Council/United Kingdom
- 206046/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- DH_/Department of Health/United Kingdom
- RG/19/6/34387/BHF_/British Heart Foundation/United Kingdom
- PG/14/89/31194/BHF_/British Heart Foundation/United Kingdom
- 203553/WT_/Wellcome Trust/United Kingdom
- 203553/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- NH/17/1/32725/BHF_/British Heart Foundation/United Kingdom
- MC_U120085815/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
