

Prevalence and Outcomes of D-Dimer Elevation in Hospitalized Patients With COVID-19
- PMID: 32840379
- PMCID: PMC7505147
- DOI: 10.1161/ATVBAHA.120.314872
Prevalence and Outcomes of D-Dimer Elevation in Hospitalized Patients With COVID-19
Abstract
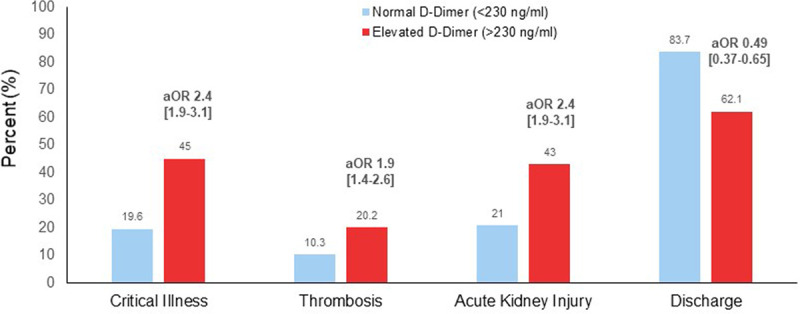
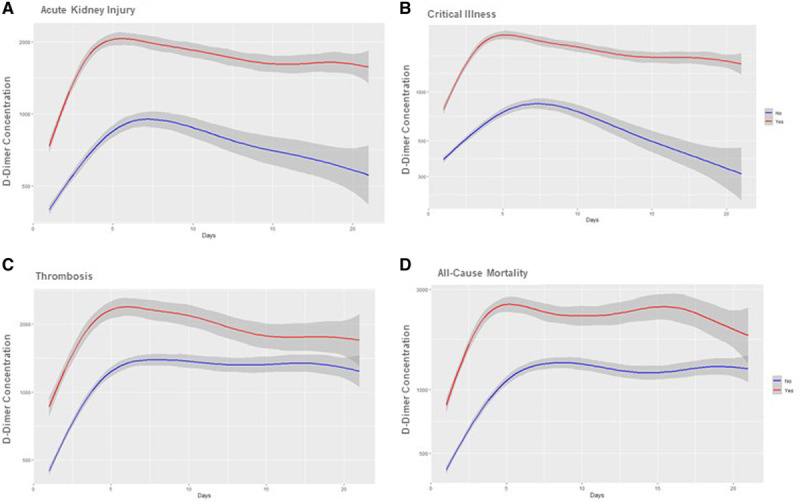
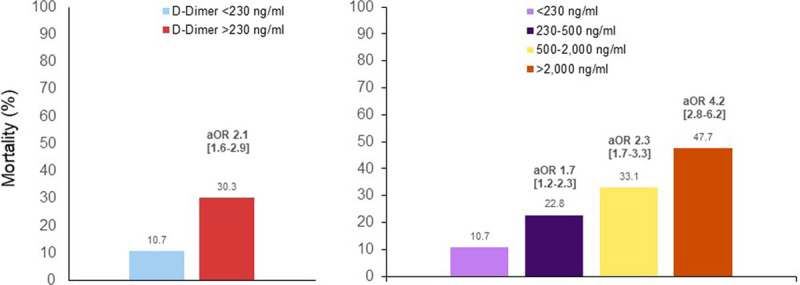
Objective: To determine the prevalence of D-dimer elevation in coronavirus disease 2019 (COVID-19) hospitalization, trajectory of D-dimer levels during hospitalization, and its association with clinical outcomes. Approach and Results: Consecutive adults admitted to a large New York City hospital system with a positive polymerase chain reaction test for SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) between March 1, 2020 and April 8, 2020 were identified. Elevated D-dimer was defined by the laboratory-specific upper limit of normal (>230 ng/mL). Outcomes included critical illness (intensive care, mechanical ventilation, discharge to hospice, or death), thrombotic events, acute kidney injury, and death during admission. Among 2377 adults hospitalized with COVID-19 and ≥1 D-dimer measurement, 1823 (76%) had elevated D-dimer at presentation. Patients with elevated presenting baseline D-dimer were more likely than those with normal D-dimer to have critical illness (43.9% versus 18.5%; adjusted odds ratio, 2.4 [95% CI, 1.9-3.1]; P<0.001), any thrombotic event (19.4% versus 10.2%; adjusted odds ratio, 1.9 [95% CI, 1.4-2.6]; P<0.001), acute kidney injury (42.4% versus 19.0%; adjusted odds ratio, 2.4 [95% CI, 1.9-3.1]; P<0.001), and death (29.9% versus 10.8%; adjusted odds ratio, 2.1 [95% CI, 1.6-2.9]; P<0.001). Rates of adverse events increased with the magnitude of D-dimer elevation; individuals with presenting D-dimer >2000 ng/mL had the highest risk of critical illness (66%), thrombotic event (37.8%), acute kidney injury (58.3%), and death (47%).
Conclusions: Abnormal D-dimer was frequently observed at admission with COVID-19 and was associated with higher incidence of critical illness, thrombotic events, acute kidney injury, and death. The optimal management of patients with elevated D-dimer in COVID-19 requires further study.
Keywords: acute kidney injury; critical illness; epidemiology; mortality; thrombosis.
Conflict of interest statement
None.
Figures
References
-
- Petrilli CM, Jones S, Yang J, Rajagopalan H, O’Donnell L, Chernyak Y, Tobin KA, Cerfolio RJ, Francois F, Horwitz LI. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020;369:m1966. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
