

Haemodynamics of Hypertension in Children
- PMID: 32840715
- PMCID: PMC7447661
- DOI: 10.1007/s11906-020-01044-2
Haemodynamics of Hypertension in Children
Abstract
Purpose of review: To review the haemodynamic characteristics of paediatric hypertension.
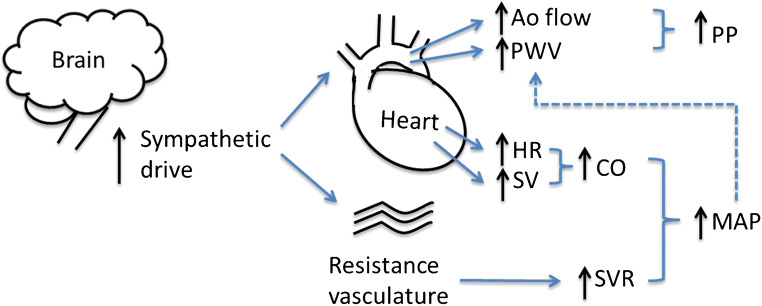
Recent findings: Pulsatile components of blood pressure are determined by left ventricular dynamics, aortic stiffness, systemic vascular resistance and wave propagation phenomena. Recent studies delineating these factors have identified haemodynamic mechanisms contributing to primary hypertension in children. Studies to date suggest a role of cardiac over activity, characterized by increased heart rate and left ventricular ejection, and increased aortic stiffness as the main haemodynamic determinants of primary hypertension in children.
Keywords: Arterial stiffness; Blood pressure; Cardiac output; Haemodynamics; Hypertension.
Conflict of interest statement
The authors declare no conflicts of interest relevant to this manuscript.
Figures
References
-
- Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, Daniels SR, et al. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics. 2017;140(3). 10.1542/peds.2017-1904. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
