

Barriers to hepatitis C direct-acting antiviral therapy among HIV/hepatitis C virus-coinfected persons
- PMID: 32840904
- PMCID: PMC7904967
- DOI: 10.1111/jgh.15228
Barriers to hepatitis C direct-acting antiviral therapy among HIV/hepatitis C virus-coinfected persons
Abstract
Background and aim: Direct-acting antivirals (DAAs) have increased hepatitis C virus (HCV) treatment opportunities for vulnerable HIV/HCV coinfected persons. The aim of this study was to identify the frequency of and potential barriers to DAA prescription in HIV/HCV patients during the first few years of DAA availability in the United States.
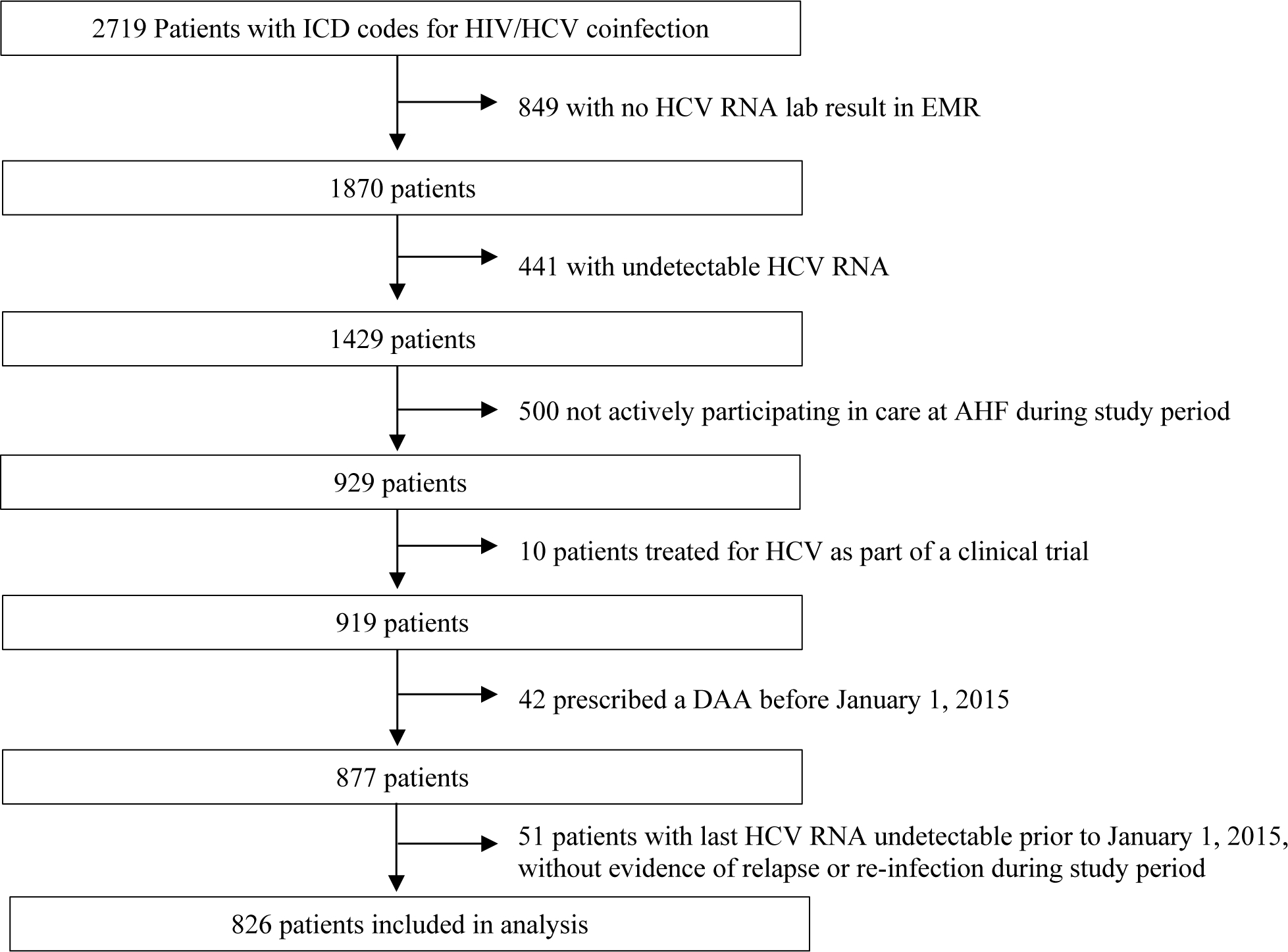
Methods: The AIDS Healthcare Foundation electronic medical record system was queried to identify all HCV viremic HIV-infected patients in care at AIDS Healthcare Foundation Healthcare centers in January 2015-August 2017 and compare characteristics by receipt of a DAA prescription. Multivariate logistic regression analyses were conducted to examine factors associated with DAA prescription.
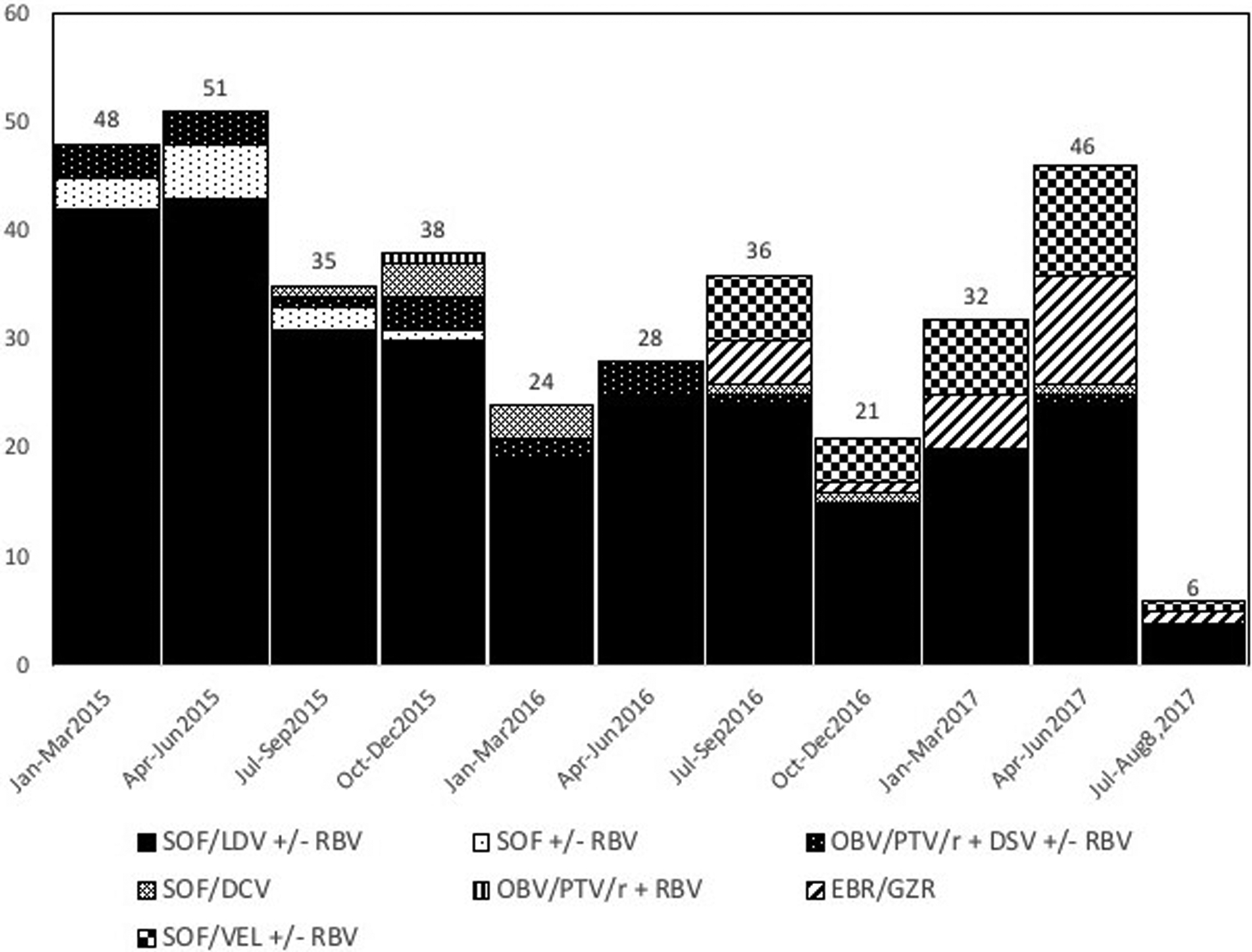
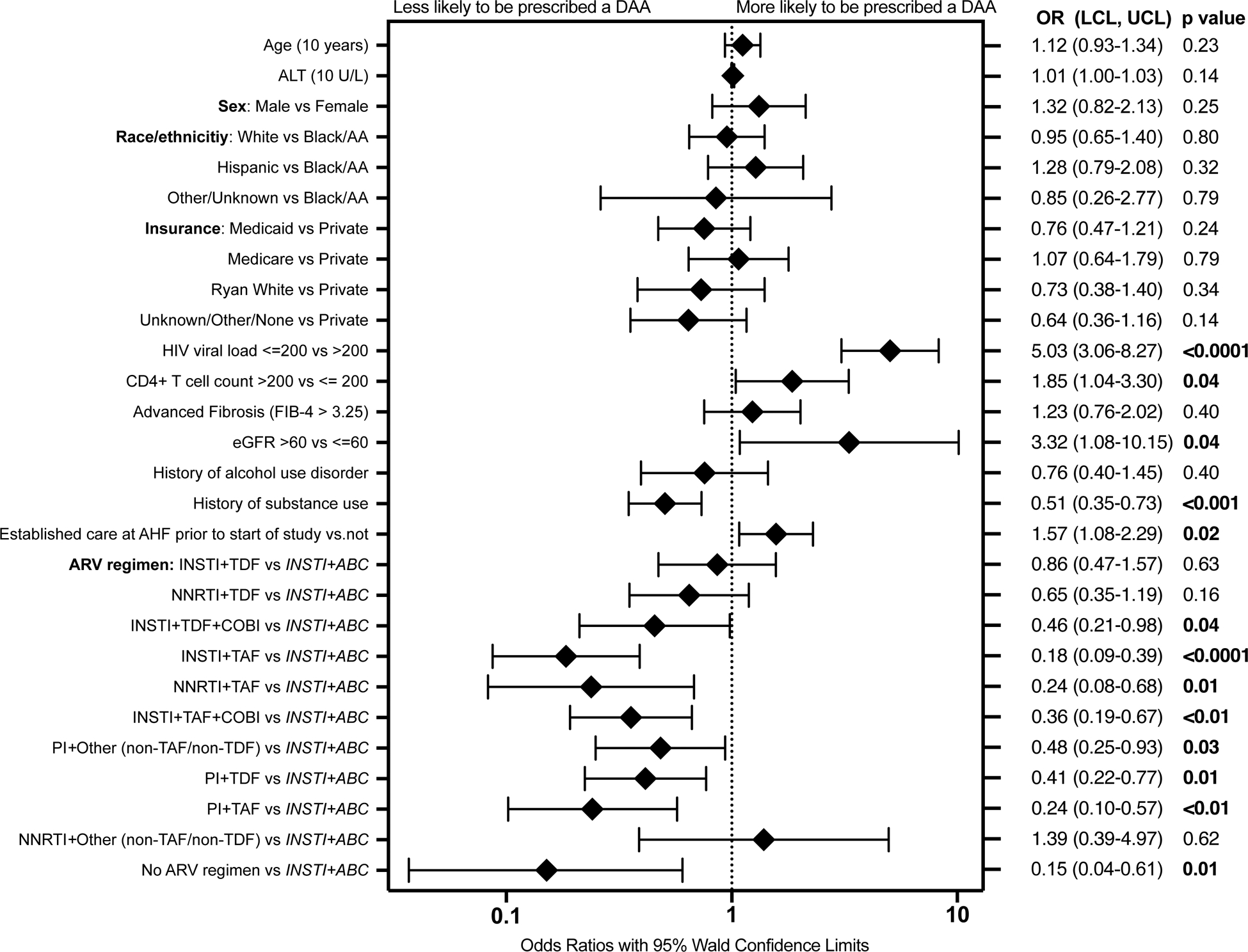
Results: Of 826 eligible patients, 355 (43%) were prescribed a DAA; among those not prescribed a DAA, 301 (64%) had well-controlled HIV (HIV RNA ≤ 200 copies per mL). In multivariate logistic regression analysis, patients with a history of substance use (odds ratio [OR], 0.51 [95% confidence interval 0.35-0.73]) or on select HIV antiretroviral regimens were less likely to be prescribed a DAA. Those who had well-controlled HIV (OR, 5.03 [3.06-8.27]), CD4 + T cell count >200 cells per mm3 (OR, 1.85 [1.04-3.30]), estimated glomerular filtration rate >60 mL/min/1.73 m2 (OR, 3.32 [1.08-10.15]), or established care prior to January 2015 (OR, 1.57 [1.08-2.29] were more likely to be prescribed a DAA.
Conclusions: In addition to lack of HIV suppression, select antiretroviral regimens, substance use, and kidney disease appeared to limit DAA prescription in the early interferon-free DAA era. Many were not prescribed DAAs despite HIV suppression. Further research is needed to determine if the observed associations persist today.
Keywords: AIDS/HIV; Access to care; Antiretroviral therapy; Direct-acting antiviral (DAA) therapy; Disparities; HCV treatment; Substance use.
© 2020 Journal of Gastroenterology and Hepatology Foundation and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
Figures
Similar articles
-
Disparities in Treatment with Direct-Acting Hepatitis C Virus Antivirals Persist Among Adults Coinfected with HIV and Hepatitis C Virus in US Clinics, 2010-2018.AIDS Patient Care STDS. 2021 Oct;35(10):392-400. doi: 10.1089/apc.2021.0087. AIDS Patient Care STDS. 2021. PMID: 34623891 Free PMC article.
-
High prevalence of willingness to use direct-acting antiviral-based regimens for hepatitis C virus (HCV) infection among HIV/HCV coinfected people who use drugs.HIV Med. 2017 Oct;18(9):647-654. doi: 10.1111/hiv.12501. Epub 2017 Mar 13. HIV Med. 2017. PMID: 28294492 Free PMC article.
-
Effectiveness and Safety of Interferon-Free Direct-Acting Antiviral Hepatitis C Virus Therapy in HIV/Hepatitis C Virus Coinfected Individuals: Results From a Pan-European Study.J Acquir Immune Defic Syndr. 2021 Feb 1;86(2):248-257. doi: 10.1097/QAI.0000000000002541. J Acquir Immune Defic Syndr. 2021. PMID: 33079903
-
Treatment of chronic HCV genotype 1 coinfection.Curr HIV/AIDS Rep. 2015 Sep;12(3):326-35. doi: 10.1007/s11904-015-0278-4. Curr HIV/AIDS Rep. 2015. PMID: 26228050 Review.
-
Management of hepatitis C virus/HIV coinfection among people who use drugs in the era of direct-acting antiviral-based therapy.Clin Infect Dis. 2013 Aug;57 Suppl 2(Suppl 2):S118-24. doi: 10.1093/cid/cit326. Clin Infect Dis. 2013. PMID: 23884059 Free PMC article. Review.
Cited by
-
Clinician barriers, perceptions, and practices in treating patients with hepatitis C virus and substance use disorder in the United States.Prev Med Rep. 2023 Feb 13;32:102138. doi: 10.1016/j.pmedr.2023.102138. eCollection 2023 Apr. Prev Med Rep. 2023. PMID: 36865395 Free PMC article.
-
Barriers and Facilitators of Hepatitis C Care in Persons Coinfected with Human Immunodeficiency Virus.Int J Environ Res Public Health. 2022 Nov 18;19(22):15237. doi: 10.3390/ijerph192215237. Int J Environ Res Public Health. 2022. PMID: 36429957 Free PMC article.
-
Perspectives on Adherence From the ACTG 5360 MINMON Trial: A Minimum Monitoring Approach With 12 Weeks of Sofosbuvir/Velpatasvir in Chronic Hepatitis C Treatment.Clin Infect Dis. 2023 Jun 8;76(11):1959-1968. doi: 10.1093/cid/ciad034. Clin Infect Dis. 2023. PMID: 36694361 Free PMC article.
References
-
- WHO | HIV and hepatitis coinfections [Internet]. [cited 2020 Feb 27]. Available from: https://www.who.int/hiv/topics/hepatitis/hepatitisinfo/en/
-
- Thein H-H, Yi Q, Dore GJ, Krahn MD. Natural history of hepatitis C virus infection in HIV-infected individuals and the impact of HIV in the era of highly active antiretroviral therapy: a meta-analysis. AIDS Lond Engl. 2008. October 1;22(15):1979–91. - PubMed
-
- de Lédinghen V, Barreiro P, Foucher J, Labarga P, Castéra L, Vispo ME, et al. Liver fibrosis on account of chronic hepatitis C is more severe in HIV-positive than HIV-negative patients despite antiretroviral therapy. J Viral Hepat. 2008. June;15(6):427–33. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
