

A prospective cohort study of Cutaneous Leishmaniasis due to Leishmania major: Dynamics of the Leishmanin skin test and its predictive value for protection against infection and disease
- PMID: 32841284
- PMCID: PMC7473511
- DOI: 10.1371/journal.pntd.0008550
A prospective cohort study of Cutaneous Leishmaniasis due to Leishmania major: Dynamics of the Leishmanin skin test and its predictive value for protection against infection and disease
Abstract
Background: Leishmanin Skin Test (LST) is considered as a useful indicator of past infection by Leishmania parasites. However, the temporal dynamics of a positive LST under different epidemiologic scenarios and whether it relates to the protection against the recurrence of an overt disease are not fully documented.
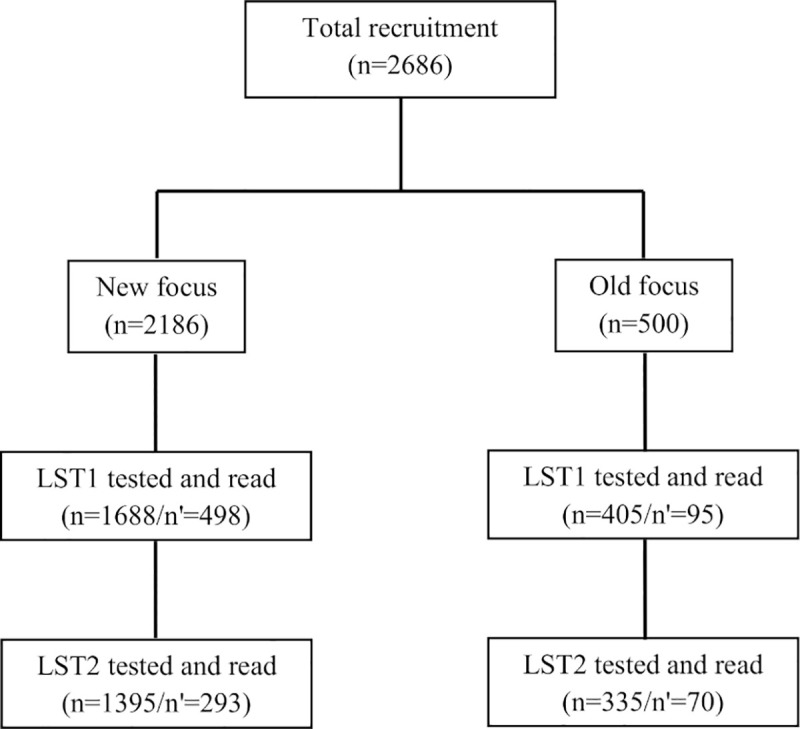
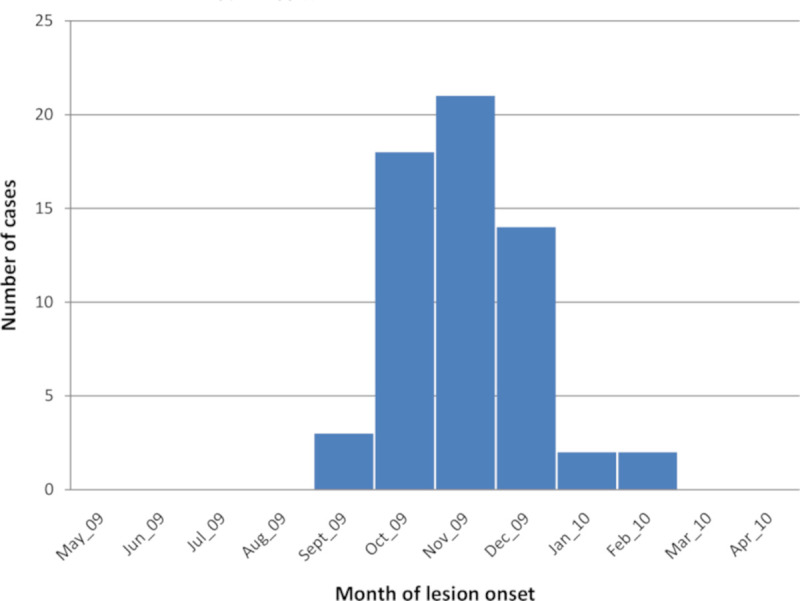
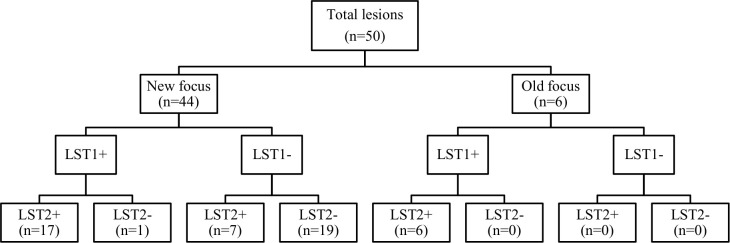
Methodology/principal findings: We report here on a population based prospective study conducted on 2686 individuals living in two foci located in Central Tunisia, to assess over a one-year epidemiologic season, the incidence of Leishmania (L.) major infection and disease and changes in LST reactivity. The two foci were both endemic for Cutaneous Leishmaniasis (CL) due to L. major, but contrasted in their history for this disease (ie: an old focus versus a recent focus). We found that most infections occurred in the new focus (290/1000; 95% CI: 265-315 person-years) with an incidence rate of CL lesions 2.4 times higher than in the old focus. Likewise, the rates of LST reactivity reversion and loss, in the new focus, were 99/1000[38-116] person-years and 14/1000[8-21] person-years, respectively. Loss of LST reactivity was not noticed in the old focus. Interestingly, the incidence rates of symptomatic infection did not differ significantly according to the LST status at enrolment (negative versus positive) between the combined foci and the new one.
Conclusions/significance: Our findings confirm LST as a good tool for assessing L. major cryptic infection. However, the instability of the LST positivity in new foci should be considered as an important confounder of the outcome of this infection when developing a research protocol for vaccine trial.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Montenegro J. Cutaneous reaction in leishmaniasis. Archives of Dermatology and Syphilology. 1926;13(2):187–94.
-
- Salah AB, Louzir H, Chlif S, Mokni M, Zaâtour A, Raouène M, et al. The predictive validity of naturally acquired delayed-type hypersensitivity to leishmanin in resistance to Leishmania major–associated cutaneous leishmaniasis. Journal of Infectious Diseases. 2005;192(11):1981–7. 10.1086/498042 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
