

Influenza A virus exposure may cause increased symptom severity and deaths in coronavirus disease 2019
- PMID: 32842015
- PMCID: PMC7575176
- DOI: 10.1097/CM9.0000000000000966
Influenza A virus exposure may cause increased symptom severity and deaths in coronavirus disease 2019
Abstract
Background: The coronavirus disease 2019 (COVID-19) outbreak occurred during the flu season around the world. This study aimed to analyze the impact of influenza A virus (IAV) exposure on COVID-19.
Methods: Seventy COVID-19 patients admitted to the hospital during January and February 2020 in Wuhan, China were included in this retrospective study. Serum tests including respiratory pathogen immunoglobulin M (IgM) and inflammation biomarkers were performed upon admission. Patients were divided into common, severe, and critical types according to disease severity. Symptoms, inflammation indices, disease severity, and fatality rate were compared between anti-IAV IgM-positive and anti-IAV IgM-negative groups. The effects of the empirical use of oseltamivir were also analyzed in both groups. For comparison between groups, t tests and the Mann-Whitney U test were used according to data distribution. The Chi-squared test was used to compare disease severity and fatality between groups.
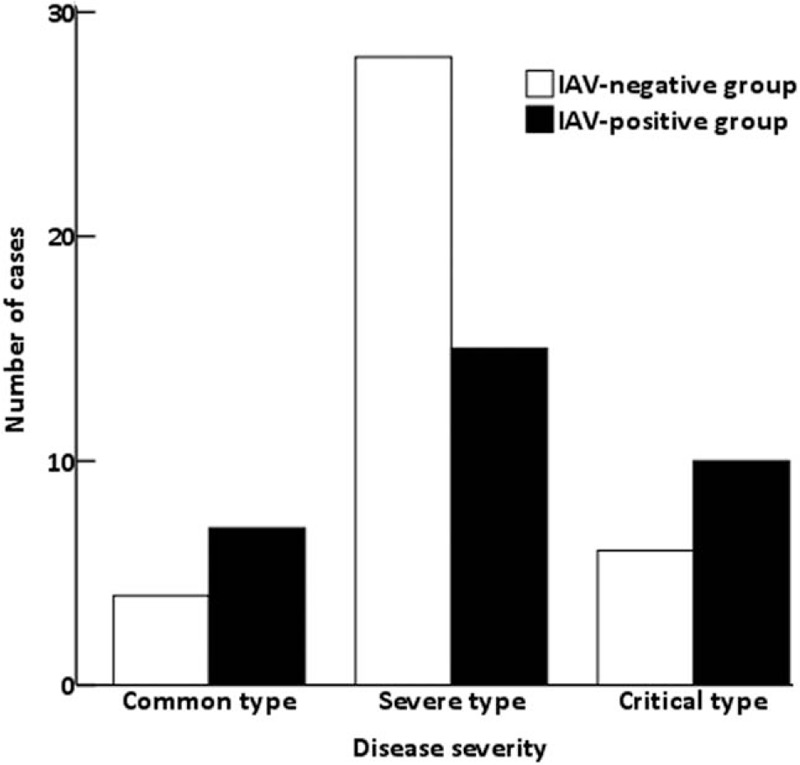
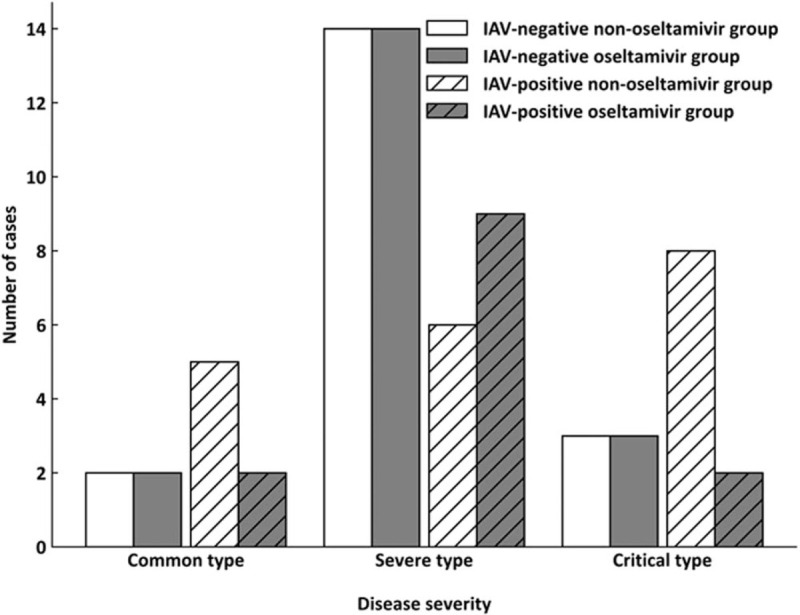
Results: Thirty-two (45.71%) of the 70 patients had positive anti-IAV IgM. Compared with the IAV-negative group, the positive group showed significantly higher proportions of female patients (59.38% vs. 34.21%, χ = 4.43, P = 0.035) and patients with fatigue (59.38% vs. 34.21%, χ = 4.43, P = 0.035). The levels of soluble interleukin 2 receptor (median 791.00 vs. 1075.50 IU/mL, Z = -2.70, P = 0.007) and tumor necrosis factor α (median 10.75 vs. 11.50 pg/mL, Z = -2.18, P = 0.029) were significantly lower in the IAV-positive group. Furthermore, this group tended to have a higher proportion of critical patients (31.25% vs. 15.79%, P = 0.066) and a higher fatality rate (21.88% vs. 7.89%, P = 0.169). Notably, in the IAV-positive group, patients who received oseltamivir had a significantly lower fatality rate (0 vs. 36.84%, P = 0.025) compared with those not receiving oseltamivir.
Conclusions: The study suggests that during the flu season, close attention should be paid to the probability of IAV exposure in COVID-19 patients. Prospective studies with larger sample sizes are needed to clarify whether IAV increases the fatality rate of COVID-19 and to elucidate any benefits of empirical usage of oseltamivir.
Conflict of interest statement
None.
Figures
Similar articles
-
Clinical characteristics of fatal and recovered cases of coronavirus disease 2019 in Wuhan, China: a retrospective study.Chin Med J (Engl). 2020 Jun 5;133(11):1261-1267. doi: 10.1097/CM9.0000000000000824. Chin Med J (Engl). 2020. PMID: 32209890 Free PMC article.
-
Serum IgM against SARS-CoV-2 correlates with in-hospital mortality in severe/critical patients with COVID-19 in Wuhan, China.Aging (Albany NY). 2020 Jul 6;12(13):12432-12440. doi: 10.18632/aging.103417. Epub 2020 Jul 6. Aging (Albany NY). 2020. PMID: 32628642 Free PMC article.
-
Analysis of adjunctive serological detection to nucleic acid test for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection diagnosis.Int Immunopharmacol. 2020 Sep;86:106746. doi: 10.1016/j.intimp.2020.106746. Epub 2020 Jun 26. Int Immunopharmacol. 2020. PMID: 32619956 Free PMC article.
-
Clinical characteristics and outcome of influenza virus infection among adults hospitalized with severe COVID-19: a retrospective cohort study from Wuhan, China.BMC Infect Dis. 2021 Apr 12;21(1):341. doi: 10.1186/s12879-021-05975-2. BMC Infect Dis. 2021. PMID: 33845787 Free PMC article.
-
Co-infection of SARS-COV-2 and Influenza A Virus: A Case Series and Fast Review.Curr Med Sci. 2021 Feb;41(1):51-57. doi: 10.1007/s11596-021-2317-2. Epub 2021 Feb 13. Curr Med Sci. 2021. PMID: 33582905 Free PMC article. Review.
Cited by
-
Viral reactivations and co-infections in COVID-19 patients: a systematic review.BMC Infect Dis. 2023 Apr 26;23(1):259. doi: 10.1186/s12879-023-08117-y. BMC Infect Dis. 2023. PMID: 37101275 Free PMC article.
-
Multidisciplinary recommendations for the management of CAR-T recipients in the post-COVID-19 pandemic era.Exp Hematol Oncol. 2023 Jul 27;12(1):66. doi: 10.1186/s40164-023-00426-x. Exp Hematol Oncol. 2023. PMID: 37501090 Free PMC article. Review.
-
COVID-19 and Influenza Co-infection: A Systematic Review and Meta-Analysis.Front Med (Lausanne). 2021 Jun 25;8:681469. doi: 10.3389/fmed.2021.681469. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34249971 Free PMC article.
References
-
- Weekly influenza reports in China. Chinese National Influenza Center, 2019. Available from: http://ivdc.chinacdc.cn/cnic/zyzx/. [Accessed February 28, 2020]
-
- Diagnosis and treatment protocol for novel coronavirus pneumonia (Pilot Edition 6). National Health Commission of the People's Republic of China, 2020. Available from: http://www.nhc.gov.cn/yzygj/s7653p/202002/8334a8326dd94d329df351d7da8aef.... [Accessed February 28, 2020]
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
