

The impact of revised diagnostic criteria on hospital trends in gestational diabetes mellitus rates in a high income country
- PMID: 32843025
- PMCID: PMC7449010
- DOI: 10.1186/s12913-020-05655-y
The impact of revised diagnostic criteria on hospital trends in gestational diabetes mellitus rates in a high income country
Abstract
Objective: In 2010, national guidelines were published in Ireland recommending more sensitive criteria for the diagnosis of Gestational Diabetes Mellitus (GDM). The criteria were based on the 2008 Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) Study and were endorsed subsequently by the World Health Organization (WHO). Screening nationally is selective based on risk factors. We examined the impact of the new criteria on hospital trends nationally for GDM over the 10 years 2008-17.
Research design and methods: Data from three national databases, the Hospital Inpatient Enquiry System (HIPE), National Perinatal Reporting System (NPRS) and the Irish Maternity Indicator System (IMIS), were analyzed using descriptive statistics, analysis of variance, and Poisson loglinear modelling.
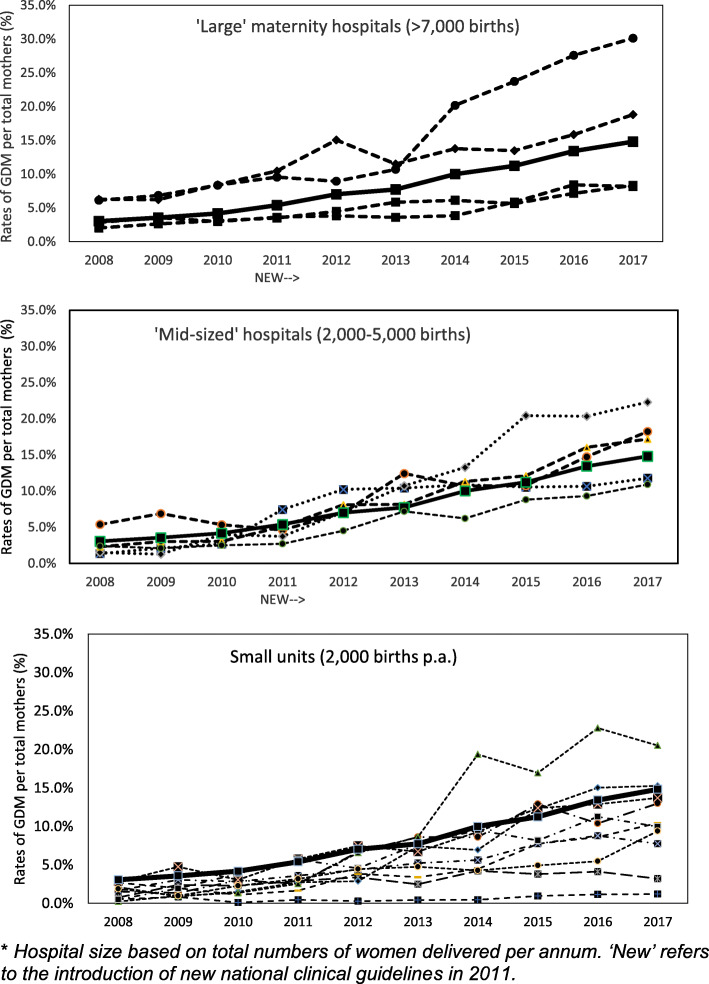
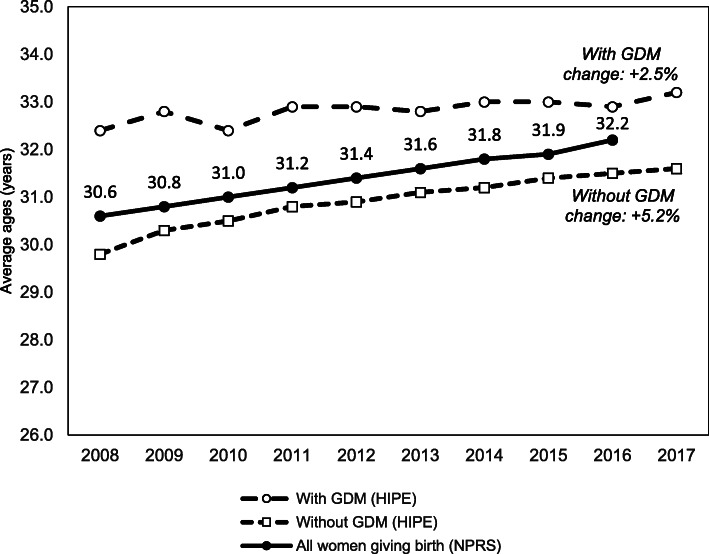
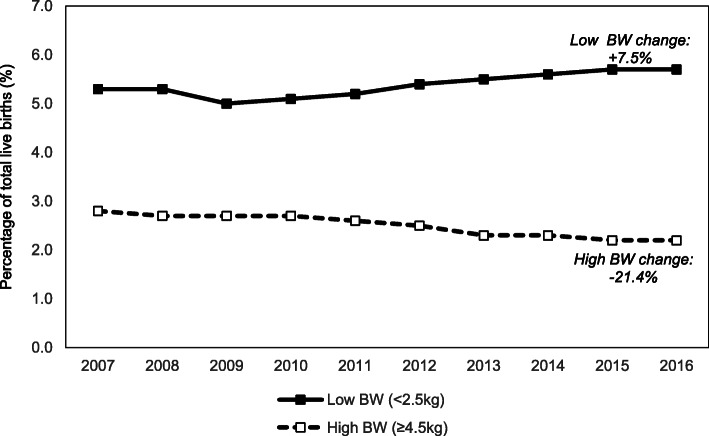
Results: The overall incidence of GDM nationally increased almost five-fold from 3.1% in 2008 to 14.8% in 2017 (p ≤ 0.001). The incidence varied widely across maternity units. In 2008, the incidence varied from 0.4 to 5.9% and in 2017 it varied from 1.9 to 29.4%. There were increased obstetric interventions among women with GDM over the decade, specifically women with GDM having increased cesarean sections (CS) and induction of labor (IOL) (p ≤ 0.001). These trends were significant in large and mid-sized maternity hospitals (p ≤ 0.001). The increase in GDM diagnosis could not be explained by an increase in maternal age nationally over the decade. The data did not include information on other risk factors such as obesity. The increased incidence in GDM diagnosis was accompanied by a decrease in high birthweight ≥ 4.5 kg nationally.
Conclusions: We found adoption of the new criteria for diagnosis of GDM resulted in a major increase in the incidence of GDM rates. Inter-hospital variations increased over the decade, which may be explained by variations in the implementation of the new national guidelines in different maternity units. It is likely to escalate further as compliance with national guidelines improves at all maternity hospitals, with implications for provision and configuration of maternity services. We observed trends that may indicate improvements for women and their offspring, but more research is required to understand patterns of guideline implementation across hospitals and to demonstrate how increased GDM diagnosis will improve clinical outcomes.
Keywords: Gestational diabetes mellitus; Oral glucose tolerance test; Pregnancy risk factors; Selective testing.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Screening and diagnosing gestational diabetes mellitus.Evid Rep Technol Assess (Full Rep). 2012 Oct;(210):1-327. Evid Rep Technol Assess (Full Rep). 2012. PMID: 24423035 Free PMC article. Review.
-
Compliance with National Institute of Health and Care Excellence risk-based screening for Gestational Diabetes Mellitus in nulliparous women.Eur J Obstet Gynecol Reprod Biol. 2016 Apr;199:60-5. doi: 10.1016/j.ejogrb.2016.01.044. Epub 2016 Feb 8. Eur J Obstet Gynecol Reprod Biol. 2016. PMID: 26901398
-
The incidence of gestational diabetes mellitus before and after the introduction of HAPO diagnostic criteria.Ceska Gynekol. 2019 Winter;84(6):404-411. Ceska Gynekol. 2019. PMID: 31948247 English.
-
Influence of different diagnostic criteria on gestational diabetes mellitus incidence and medical expenditures in China.J Diabetes Investig. 2019 Sep;10(5):1347-1357. doi: 10.1111/jdi.13008. Epub 2019 Feb 27. J Diabetes Investig. 2019. PMID: 30663279 Free PMC article.
-
The interplay between maternal obesity and gestational diabetes mellitus.J Perinat Med. 2015 May;43(3):311-7. doi: 10.1515/jpm-2014-0272. J Perinat Med. 2015. PMID: 25389982 Review.
Cited by
-
Evolution of Gestational Diabetes Mellitus across Continents in 21st Century.Int J Environ Res Public Health. 2022 Nov 28;19(23):15804. doi: 10.3390/ijerph192315804. Int J Environ Res Public Health. 2022. PMID: 36497880 Free PMC article. Review.
-
Abnormal glucose tolerance in women with prior gestational diabetes mellitus: a 4-year follow-up study.Ir J Med Sci. 2023 Apr;192(2):641-648. doi: 10.1007/s11845-022-03005-x. Epub 2022 Apr 13. Ir J Med Sci. 2023. PMID: 35419723
-
Gestational diabetes mellitus and subsequent cardiovascular disease in a period of rising diagnoses: Cohort study.Acta Obstet Gynecol Scand. 2025 Feb;104(2):331-341. doi: 10.1111/aogs.15022. Epub 2025 Jan 2. Acta Obstet Gynecol Scand. 2025. PMID: 39744821 Free PMC article.
-
Experiences of Postpartum Follow-Up and Participation in a Lifestyle Intervention after Gestational Diabetes: A Qualitative Study.Nutrients. 2024 Oct 15;16(20):3487. doi: 10.3390/nu16203487. Nutrients. 2024. PMID: 39458482 Free PMC article.
-
Non-diabetic fetal macrosomia: outcomes of elective delivery versus expectant management.Ir J Med Sci. 2023 Jun;192(3):1249-1257. doi: 10.1007/s11845-022-03076-w. Epub 2022 Jul 4. Ir J Med Sci. 2023. PMID: 35781860 Free PMC article.
References
-
- HAPO Study Cooperative Research Group. Metzger BF, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR, Hadden DR, et al. Hyperglycemia and Adverse Pregnancy Outcomes. N Engl J Med. 2008;358(19):1991–2002. - PubMed
-
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel. Metzger BE, Gabbe SG, Persson B, Buchanan TA, Catalano PA, Damm P, Dyer AR, et al. International association of diabetes and pregnancy study groups recommendation on the diagnosis and classification of hyperglycaemia in pregnancy. Diabetes Care. 2010;33(3):676–682. doi: 10.2337/dc09-1848. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
