

Prospective validation of classification of intraoperative adverse events (ClassIntra): international, multicentre cohort study
- PMID: 32843333
- PMCID: PMC7500355
- DOI: 10.1136/bmj.m2917
Prospective validation of classification of intraoperative adverse events (ClassIntra): international, multicentre cohort study
Erratum in
-
Prospective validation of classification of intraoperative adverse events (ClassIntra): international, multicentre cohort study.BMJ. 2025 Jan 22;388:r117. doi: 10.1136/bmj.r117. BMJ. 2025. PMID: 39843180 Free PMC article. No abstract available.
Abstract
Objective: To prospectively assess the construct and criterion validity of ClassIntra version 1.0, a newly developed classification for assessing intraoperative adverse events.
Design: International, multicentre cohort study.
Setting: 18 secondary and tertiary centres from 12 countries in Europe, Oceania, and North America.
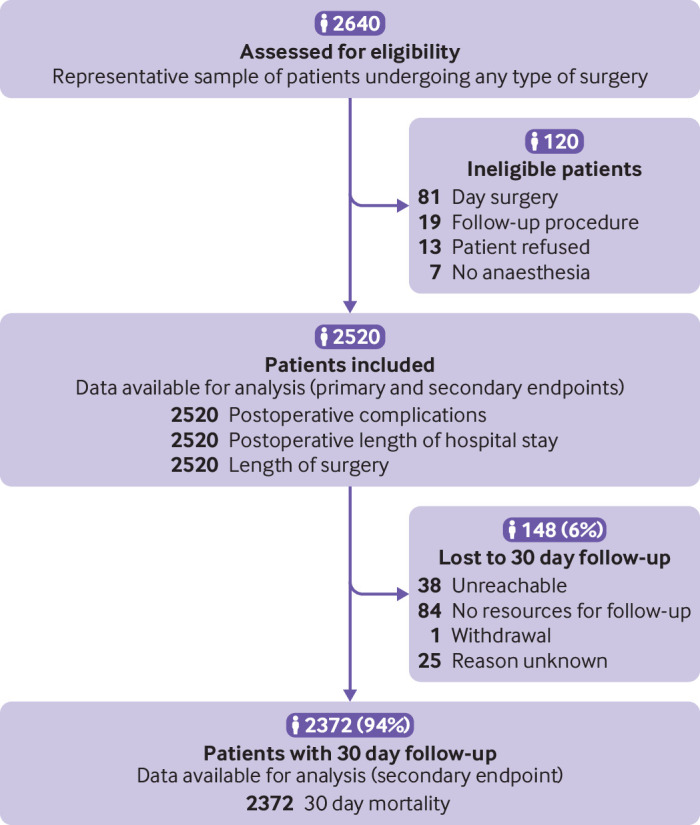
Participants: The cohort study included a representative sample of 2520 patients in hospital having any type of surgery, followed up until discharge. A follow-up to assess mortality at 30 days was performed in 2372 patients (94%). A survey was sent to a representative sample of 163 surgeons and anaesthetists from participating centres.
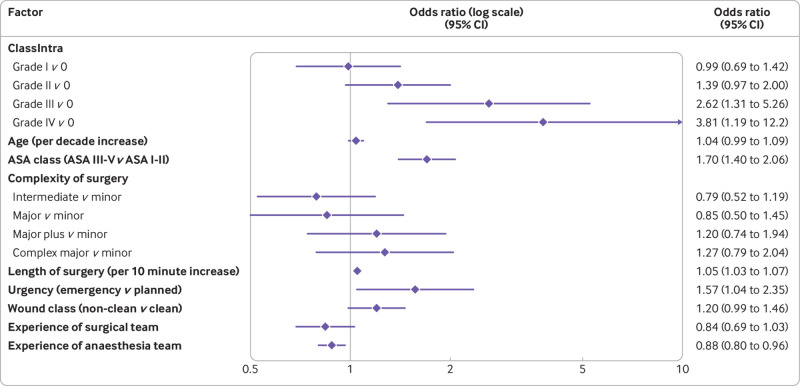
Main outcome measures: Intraoperative complications were assessed according to ClassIntra. Postoperative complications were assessed daily until discharge from hospital with the Clavien-Dindo classification. The primary endpoint was construct validity by investigating the risk adjusted association between the most severe intraoperative and postoperative complications, measured in a multivariable hierarchical proportional odds model. For criterion validity, inter-rater reliability was evaluated in a survey of 10 fictitious case scenarios describing intraoperative complications.
Results: Of 2520 patients enrolled, 610 (24%) experienced at least one intraoperative adverse event and 838 (33%) at least one postoperative complication. Multivariable analysis showed a gradual increase in risk for a more severe postoperative complication with increasing grade of ClassIntra: ClassIntra grade I versus grade 0, odds ratio 0.99 (95% confidence interval 0.69 to 1.42); grade II versus grade 0, 1.39 (0.97 to 2.00); grade III versus grade 0, 2.62 (1.31 to 5.26); and grade IV versus grade 0, 3.81 (1.19 to 12.2). ClassIntra showed high criterion validity with an intraclass correlation coefficient of 0.76 (95% confidence interval 0.59 to 0.91) in the survey (response rate 83%).
Conclusions: ClassIntra is the first prospectively validated classification for assessing intraoperative adverse events in a standardised way, linking them to postoperative complications with the well established Clavien-Dindo classification. ClassIntra can be incorporated into routine practice in perioperative surgical safety checklists, or used as a monitoring and outcome reporting tool for different surgical disciplines. Future studies should investigate whether the tool is useful to stratify patients to the appropriate postoperative care, to enhance the quality of surgical interventions, and to improve long term outcomes of surgical patients.
Trial registration: ClinicalTrials.gov NCT03009929.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the Goldschmidt-Jacobson Foundation, University of Basel, Foundation for Research and Education in Anaesthesiology, Switzerland, and VSB fonds (Verenigde Spaar Bankenfonds) for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. RR is an employee of F Hoffmann-La Roche (includes Stock-Settled Appreciation Rights). The study has no connection to her employment by the company. RR continues to be affiliated to the University of Basel.
Figures
Comment in
-
Intraoperative adverse events grading tools and their role in honest and accurate reporting of surgical outcomes.Surgery. 2022 Sep;172(3):1035-1036. doi: 10.1016/j.surg.2022.04.029. Epub 2022 May 18. Surgery. 2022. PMID: 35597615 No abstract available.
References
-
- Bainbridge D, Martin J, Arango M, Cheng D, Evidence-based Peri-operative Clinical Outcomes Research (EPiCOR) Group . Perioperative and anaesthetic-related mortality in developed and developing countries: a systematic review and meta-analysis. Lancet 2012;380:1075-81. 10.1016/S0140-6736(12)60990-8 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical