

Pregnancy Outcome Patterns of Medicaid-Eligible Women, 1999-2014: A National Prospective Longitudinal Study
- PMID: 32844103
- PMCID: PMC7416150
- DOI: 10.1177/2333392820941348
Pregnancy Outcome Patterns of Medicaid-Eligible Women, 1999-2014: A National Prospective Longitudinal Study
Abstract
Introduction: The number and outcomes of pregnancies experienced by a woman are consequential determinants of her health status. However, there is no published research comparing the patterns of subsequent pregnancy outcomes following a live birth, natural fetal loss, or induced abortion.
Objectives: The objective of this study was to describe the characteristic patterns of subsequent pregnancy outcomes evolving from each of three initiating outcome events (birth, induced abortion, natural fetal loss) occurring in a Medicaid population fully insured for all reproductive health services.
Methods: We identified 7,388,842 pregnancy outcomes occurring to Medicaid-eligible women in the 17 states which paid for abortion services between 1999-2014. The first known pregnancy outcome for each woman was marked as the index outcome which assigned each woman to one of three cohorts. All subsequent outcomes occurring up to the fifth known pregnancy were identified. Analyses of the three index outcome cohorts were conducted separately for all pregnancy outcomes, three age bands (<17, 17-35, 36+), and three race/ethnicity groups (Hispanic, Black, White).
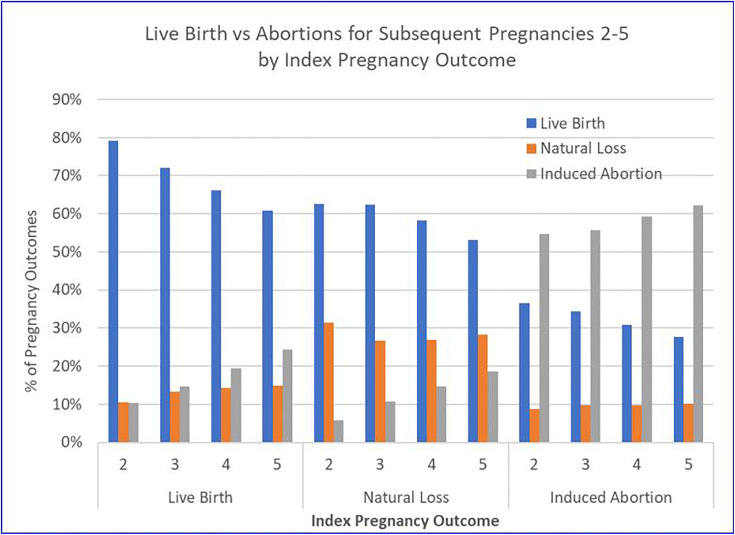
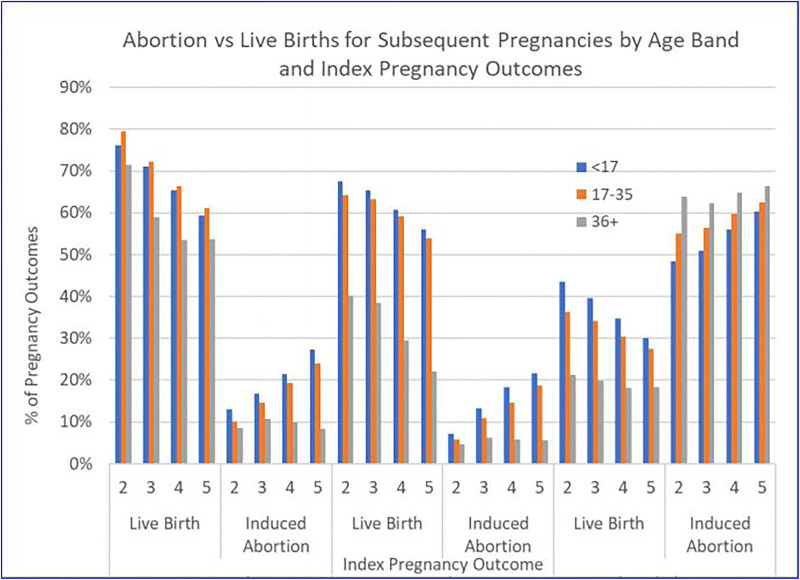
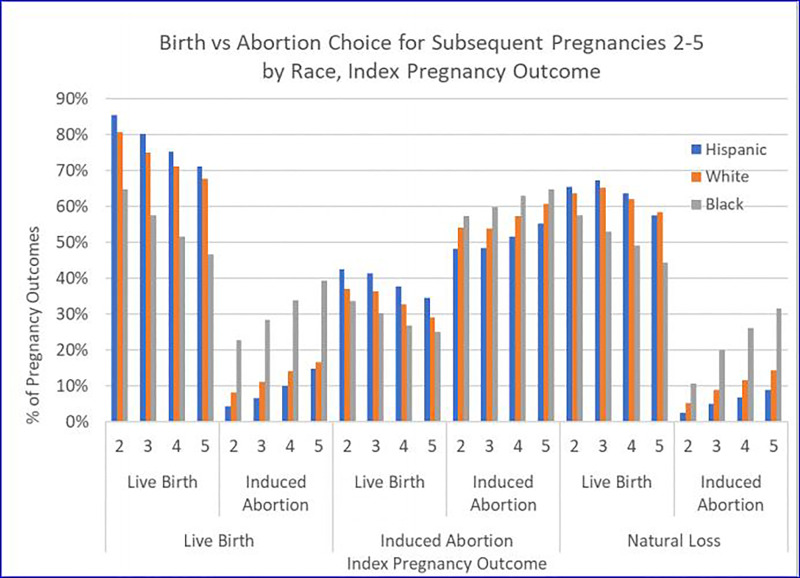
Results: Women with index abortions experienced more lifetime pregnancies than women with index births or natural fetal losses and were increasingly more likely to experience another pregnancy with each subsequent pregnancy. Women whose index pregnancy ended in abortion were also increasingly more likely to experience another abortion at each subsequent pregnancy. Both births and natural fetal losses were likely to result in a subsequent birth, rather than abortion. Women with natural losses were increasingly more likely to have a subsequent birth than women with an index birth. All age and racial/ethnic groups exhibited the characteristic pattern we have described for all pregnancy outcomes: abortion is associated with more subsequent pregnancies and abortions; births and fetal losses are associated with subsequent births. Other differences between groups are, however, apparent. Age is positively associated with the likelihood of a birth following an index birth, but negatively associated with the likelihood of a birth following an index abortion. Hispanic women are always more likely to have a birth and less likely to have an abortion than Black or White women, for all combinations of index outcome and the number of subsequent pregnancies. Similarly, Black women are always more likely to have an abortion and less likely to experience a birth than Hispanic or White women.
Conclusion: Women experiencing repeated pregnancies and subsequent abortions following an index abortion are subjected to an increased exposure to hemorrhage and infection, the major causes of maternal mortality, and other adverse consequences resulting from multiple separation events.
Keywords: Medicaid; induced abortion; natural fetal loss; pregnancy outcomes.
© The Author(s) 2020.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Zhou W, Nielsen GL, Larsen H, Olsen J. Induced abortion and placenta complications in the subsequent pregnancy. Acta Obstet Gynecol Scand. 2001;80(12):1115–1120. doi:10.1034/j.1600-0412.2001.801207.x - PubMed
-
- Heidam LZ. Spontaneous abortions among factory workers: the importance of gravidity control. Scand J Soc Med. 1983;11(3):81–85. - PubMed
LinkOut - more resources
Full Text Sources
